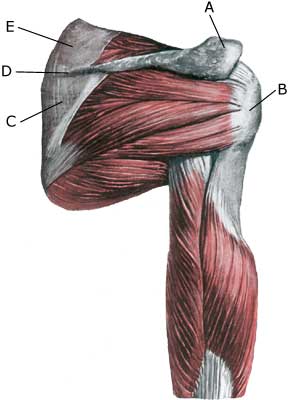
RUPTURE OF THE LOWER SHOULDER BLADE MUSCLE
|
||
|
||
| Cause: When a muscle is suddenly subjected to a load in excess of the strength of the muscle, a rupture will occur in the muscle. Rupture of the infraspinatus (the lower shoulder blade muscle) is a common throwing injury (handball). Inflammation of the tendon (tendinitis) often precede larger ruptures and tendinitis is not rare combined with inflammation of the bursa (bursitis subacromialis).
Symptoms: In light cases a local tenderness is felt after the load (“muscle strain”, “imminent pulled muscle”, “inflammation of the tendon”), which can precede larger ruptures if the exercise intensity is not altered. In severe cases a sudden shooting pains are felt in the muscle (“partial muscle rupture”, “pulled muscle”) and in the worst case a violent snap is felt, rendering the muscle unusable (“total muscle rupture”). In case of muscle damage the following three symptoms are characteristic: pain upon pressure (externally, on the back of the shoulder), stretching and activation against resistance (rotation outwards against resistance). Acute treatment: Click here. Examination: In light cases with only minimal tenderness medical examination is not necessarily required. In case of more pronounced pain and in lack of progress a medical examination should be carried out to ensure the correctness of the diagnosis and to commence the correct treatment (article-1) (article-2). A normal medical examination is usually sufficient in order to make the diagnosis, however, if there is any doubt concerning the diagnosis the medical examination should be supplemented with an ultrasound scan, which is the most suitable examination for shoulder damage (Ultrasonic image) (article). Treatment: The treatment primarily involves relief from the pain inducing activity, stretching and rehabilitation of the muscles around the shoulder. In light cases with slowly insetting tenderness after load, without the sensation of a snap and good function of the muscle (“muscle strain”, “imminent pulled muscle”, “inflammation of the tendon”), medical treatment in the form of rheumatic medicine (NSAID) or injection of corticosteroid (usually in the subacromiale bursa over the infraspinatus muscle). Since the injection of corticosteroider is part of a long-term rehabilitation of a long-term injury, it is often necessary for rehabilitation to stretch over several weeks to months to reduce the risk of recurrences and ruptures. The tendon can of course not sustain maximum load after a prolonged injury-period and only a short-term rehabilitation period. Ultrasound guided injection gives the maximal effect with minimal risk, since “blind” injections hit the wrong structures in more than half the cases (article). In case of lack of progress in rehabilitation and medical treatment, an operative treatment can be attempted. Complications: If progress is not smooth, it should be considered whether the diagnosis is correct or whether complications have arisen. Amongst others the following should be considered:
|