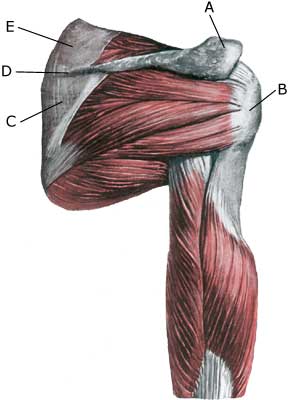
BRISTNING AF ØVRE SKULDERBLADSMUSKEL
|
||
|
||
| Cause: With age and repeated loads with the arm above the head (tennis, swimming) the upper shoulder blade muscle tendon (M supraspinatus) becomes stiffer and less flexible, and is more easily squeezed between the head of the upper arm (caput humeri) and the acromion, causing the tendon to become frayed and weakened with risk of ruptures. When a muscle is suddenly subjected to a load in excess of the strength of the muscle, a rupture occurs (fall on an outstretched arm, lifting or throwing of heavy objects). The vast majority of ruptures are partial muscle ruptures. The vast majority of total ruptures are seen in older people with wear and tear changes in the muscle tendon (in very old people total ruptures are very frequent). It is very rare for healthy tendons to rupture.
Symptoms: In light cases a local tenderness is felt after the load (“muscle strain”, “imminent pulled muscle”). In severe cases a sudden shooting pain in the muscle is felt (partial “muscle rupture” or “pulled muscle”) and in the worst case a sudden snap is felt, rendering the muscle unusable (“total muscle rupture”). With muscle damage the following three symptoms are characteristic: pain upon pressure, stretching (hand to the loin) and activation against resistance (lifting the arm to the side or above the head). The pain is localized on top and external to the shoulder. After a longer period, loss of muscle can be observed on the back of the shoulder blade. With many older people the rupture has not produced symptoms. Acute treatment: Click here. Examination: Light cases with only minimal tenderness do not necessarily require medical examination. In case of more pronounced pain or trouble lifting the arm away from the body and in case of lack of progress, a medical examination should be carried out to ensure the correct diagnosis and treatment. Ordinary medical examination is often sufficient to make the diagnosis (article-1) (article-2). Returning to the bedside: using the history and physical examination to identify rotator cuff tears, 2) The ‘dropping’ and ‘hornblower’s’ signs in evaluation of rotator cuff tears. If there is uncertainty about the diagnosis it should be supplemented with ultrasound, which is the most suitable examination for shoulder injuries (article) (Ultrasonic image). If there is doubt as to whether it is a total or partial rupture, the doctor can inject a local anaesthetic around the rupture. If, after this, the arm is able to move freely, it is not a total rupture (diagnostic blockade). Treatment: Only in cases of near total rupture of the supraspinatus muscle can surgery be considered. Renewed ruptures occur relatively frequently after surgery (article). In partial ruptures and total ruptures in the elderly the treatment is short-term relief and careful rehabilitation of the part of the supraspinatus muscle, which has not ruptured. Complications: If progress is not smooth, it should be considered whether the diagnosis is correct or whether complications have arisen. Amongst others the following should be considered:
|