|
Anatomic basis of chronic groin pain with special reference to sports hernia. |
Alle indlæg af urtehave_com
treatment-article1
|
Surgical management of groin pain of neural origin. STUDY DESIGN. RESULTS. CONCLUSIONS. |
cause-article1
|
The sportsman’s hernia–fact or fiction? |
examination-article
|
Sportsman’s hernia. METHODS. RESULTS. CONCLUSION. |
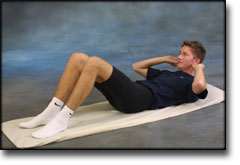
step4
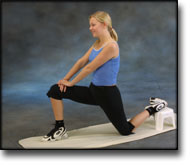
Training ladder for:
“SPORTSMAN’S HERNIA”
(SPORTSMANN’S HERNIA)
STEP 4 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


























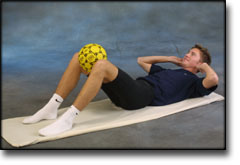
step3
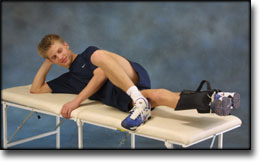
Training ladder for:
“SPORTSMAN’S HERNIA”
(SPORTSMANN’S HERNIA)
STEP 3 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

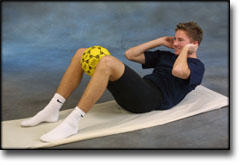
step2
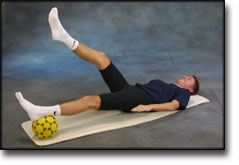
Training ladder for:
“SPORTSMAN’S HERNIA”
(SPORTSMANN’S HERNIA)
STEP 2 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||





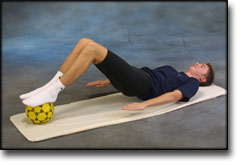
step1
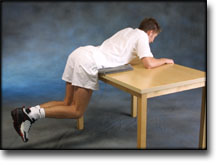
Training ladder for:
“SPORTSMAN’S HERNIA”
(SPORTSMANN’S HERNIA)
STEP 1 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||







step4
Training ladder for:
RUPTURE OF THE ADDUCTOR MUSCLE OF THE THIGH
(RUPTURA M ADDUKTOR LONGUS)
STEP 4 |
Unlimited: Cycling. Swimming. Running on a soft surface.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step3
Training ladder for:
RUPTURE OF THE ADDUCTOR MUSCLE OF THE THIGH
(RUPTURA M ADDUKTOR LONGUS)
STEP 3 |
Unlimited: Cycling. Swimming. Jogging on a soft surface without sudden directional change.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |