|
Defects of pars interarticularis in athletes: a protocol for nonoperative treatment. |
Kategoriarkiv: Fracture of the vertebral arch
Examination-a1
|
Spondylolysis and spondylolisthesis in the pediatric and adolescent population. |
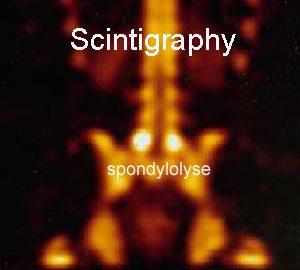
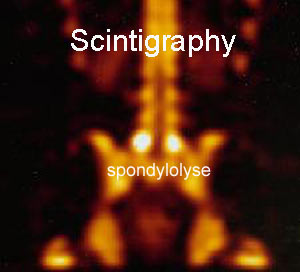
Scintigraphy
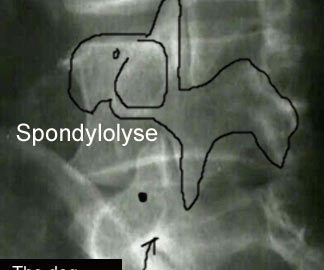
X-Ray

Cause-a2
|
Lumbar spondylolysis and spondylolisthesis in college football players. A prospective study. |
Cause-a1
|
Lumbar spondylolysis in children and adolescents. We investigated 185 adolescents under the age of 19 years with spondylolysis. All but five were active in sport. The pars defect was classified into early, progressive and terminal stages. Of the 346 pars defects in 185 patients, 39.6% were early, 29.5% progressive and 30.9% in the terminal stages. Conservative management produced healing in 73.0% of the early, 38.5% of the progressive and none of the terminal defects. These results suggest that spondylolysis is caused by repetitive microtrauma during growth and can be successfully treated conservatively if treatment is started in the early stage. There was elongation of the pars interarticularis as the pars defect progressed, and this is likely to be a consequence of the defect rather than a contributing cause. |

sketch