|
Work-related upper extremity musculoskeletal disorders. |
Kategoriarkiv: Hand

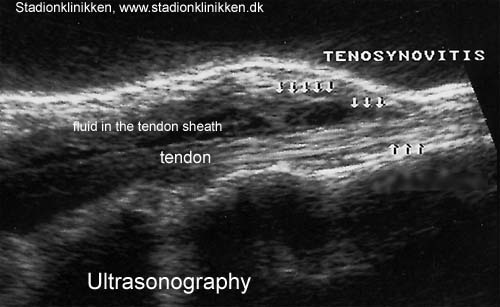
ultrasonic-image
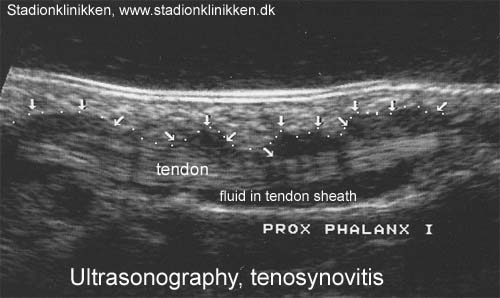
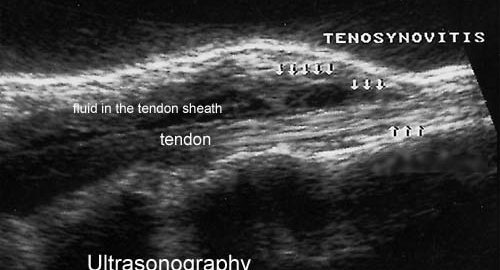
ultrasonic-image
examination-article
SportNetDoc
|
Sonography of the hand and wrist. |
cause-article2
|
Rupture of the extensor pollicis longus tendon. |
cause-article1
|
Incidence and causes of tenosynovitis of the wrist extensors in long distance paddle canoeists. METHOD. RESULTS. CONCLUSION. |
examination-article
|
Usefulness of high resolution US in the evaluation of effusion in osteoarthritic first carpometacarpal joint. METHODS. RESULTS. CONCLUSIONS. |
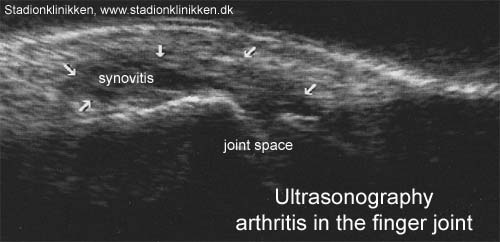
ultrasonic-image
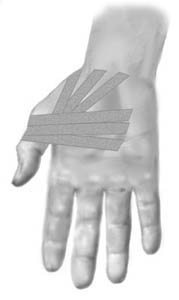
tape-instruction
Objective: Stabilise the metacarpophalangeal joint (MCP1 joint) |
|||
 |
|||
| Application: The thumb should be held in a neutral position. Start in the middle of the palm adjacent to the wrist, draw the tape around the thumb’s metacarpophalangeal joint and return to the palm and cross the start tape (A). The next tape is applied in similar fashion, but started slightly further out on the palm (B). A third strip can be applied in a continued fan formation. (C). |
treatment-article2
|
Role of MR imaging in the management of “skier’s thumb” injuries. |