|
Rupture of the tibial tuberosity in children and adolescents. |
Kategoriarkiv: Osgood-Schlatter desease
Treatment(2)
|
Local corticosteroid injection in sport: review of literature and guidelines for treatment. Abstract. The risks and benefits of local injection therapy of overuse sports injuries with corticosteroids are reviewed. Injection of corticosteroid inside the tendon has a deleterious effect on the tendon tissue and should be unanimously condemned. There exists no reliable proof of the deleterious effects of peritendinous injections. Too many conclusions in the literature are based on poor scientific evidence and it is just the reiteration of a dogma if all steroid injections are abandoned. The corticosteroids represent an adjuvant treatment in the overall management of sports injuries: Basic treatment is “active” rest and graduated rehabilitation with the limits of pain. With proper indications there are only few and trivial complications that may occur with corticosteroid injections. Guidelines for the proper local injection therapy with corticosteroids are given. Introduction. Since Hench and co-workers won the Nobel prize for medicine in 1950 for reporting the effect of the steroid hormone on the rheumatoid joint and Hollander in 1951 elucidated how steroids could be used locally with reduction of systemic side effects, the use of steroids has been one of the greatest advances in medicine in suppressing inflammation. Steroids inhibit the early aspects of the inflammatory process, i.e. edema, fibrin deposition, capillary dilatation, migration of leukocytes into the inflamed area and phagocytotic activity. In addition, steroids inhibit the later manifestations of the inflammatory process, i.e. capillary and fibroblast proliferation, deposition of collagen and, still later, scar formation. Few years later came the first evidence that steroids injected locally also had adverse effects. Candler reported rapidly progressive degenerative arthritis following intraarticular hydrocortisone injections and Mankin 4 showed diminished synthesis of articular cartilage. These initial reports were followed by many others condemning steroids and also holding them responsible for conditions such as tendon ruptures. The last 20 years have seen an explosion of interest in sport and exercise, and consequently there has been an epidemic of sports-related injuries. Soft tissue injuries are the most common problem. To day there is generally a rather good understanding of injury, healing mechanisms and rehabilitation, replacing the previous inadequate response of “bandage and rest for three weeks”. Noyes documented the beneficial effects of physical activity compared with the deterioration in the physical properties of ligaments caused by immobilization. Other reseachers have subsequently shown that immobilization is detrimental and activity beneficial in the management of injuries to ligaments 6. Inflammatory reactions that are very common in sport are often caused by overuse. These inflammatory reactions include bursitis, arthritis, tendinitis, tenosynovitis and peritendinitis. It is well known that footballers, for example, may develop symphysitis through chronic loading and radiologically there may be apparent erosive changes 7,8. Local injections of steroid in sport are used to reduce the inflammatory reactions, prevent and treat lesions with inflammation and prevent ruptures of the inflamed tendons so the athletes can return to sports before immobilization has reduced the physical properties of the soft tissues seriously. Many investigators have reported case examples of tendon ruptures, especially among athletes, from injections of corticosteroids. The question remains whether these ruptures are the effect of steroids or merely an additional manifestation of the disease for which the steroids were used. The aim of this study is to review the literature concerning the effects and adverse effects of corticosteroids and give guidelines for the injection of local corticosteroid in athletes. Cortocosteroid injections, tendon degeneration and tendon rupture. Spontaneous partial or total ruptures of the tendons are common in sport. While the risk of tendon rupture following intratendinous (inside the tendon) or peritendinous (around the tendon) injection of corticosteroid is controversial, it is well known that inflammation and degeneration can predispose to tendon ruptures. Tendon rupture in patients with inflammatory diseases as rheumatoid arthritis or systemic lupus erythematosus is a well-regnognized entity. While Vaughan-Jackson attributed tendon ruptures in patients with rheumatoid arthritis to abrasion or attrition over bony prominence, Moore in 1987 showed that direct synovial invasion and degeneration coupled with devascularization and loss of nutrition probably account for many of the tendon ruptures in rheumatoid arthritis. He did not found previous steroid injections to be causally related, although such a possibility can not be ruled out. Some authors have found that 50% of the ruptured tendon that had not received local steroid injections show macroscopically and microscopically identifiable degenerative lesion while in a report the ruptured tendons were normal. Kannus and Józsa examined 891 spontaneously ruptured tendons by light microscopy, electromicroscopy, polarization microscopy, and with enzyme histological and immunohistochemical examinations and compared them with 445 age and sex-matched nonruptured healthy control tendons of previously helaty individuals. In 97% of the spontaneously ruptured tendons, there were degenerative changes. Similar changes were found in only 34% of the control tendons (p0.001). They did not found steroid-induced lesions in the spontaneously ruptured tendons. Ljungqvist found no histological difference in tendon ruptures between those having received local corticosteroid injection and those without any history of corticosteroid injection. In two post mortem studies with 12 and 891 subjects Williams showed, contrary to Kannus and Józsa, that degenerative changes in tendons were not a part of a normal aging process. In patients with systemic inflammatory diseases, Ippolito did find degenerative changes. Many authors have, with animals, evaluated and described the effect of injection of corticosteroids into the tendon. Some authors have shown that the intratendinous injections result in collagen necrosis, followed by a decrease in tensile strength: Ferland showed 100% of the adult albino rats receiving intratendinous injection of corticosteroid directly into the Achilles tendon had localized tendon necrosis at the site of the injection. The rats receiving peritendinous injections showed, in turn, an intact structure in 95% of cases. No tendon necrosis occurred in rats injected intratendinously with an identical volume of physiologic serum. Similar results were found by Balasubramanian. In his study, necrosis was seen as early as forty-five minutes after intratendinous injection of hydrocortisone, and after eight weeks, the healing process was still incomplete. The necrosis of collagen was seen to be continuous with normal collagen fibres at the periphery of the lesion. No necrosis was seen in any of the control tendons injected with saline solution. Noyes 30 showed that a single injection into the anterior cruciate ligament of Rhesus monkeys substantially decreased the tensile strength up to one year after the injection. In monkeys which received intraarticular injections there were no changes in tensile strength or histology. Kennedy showed a decrease in tensile strength in the Achilles tendons of rabbit two and seven days after a single injection of betamethasone, but no difference in controls after two weeks. Kapetanos showed, in turn, in a group of rabbits that injection of repeated doses of local corticosteroid intratendinously significant decreased the formation of adhesions, but also decreased the tendon weight, load to failure and energy to failure, when compared to the saline-injected group. There were no significant differences in healing and strain-elongation of the tendons in the two groups. Pelps, Mackie and Matthews found no alterations in the mechanical properties in tendons of rabbit injected intratendinously with corticosteroid. Concerning peritendinous injection of corticosteroid, McWhorter described a study, where he injected hydrocortisone acetate around injured Achilles tendons of rats and found no significant difference in the mean separation forces for the damaged Achilles tendons whether given 0, 1, 3 or 5 injections at weekly intervals from one week after trauma and onwards. There was no lightmicroscopic evidence that hydrocortisone was associated with consistent reduction of cells recognized as part of the healing process when compared with control groups. He concluded that hydrocortisone acetate has no deleterious effect on the rat Achilles tendon as measured biomechanically or histologically. Regarding systemic treatment with corticosteroid studies by Francis and Randall showed that treatment with hydrocortisone acetate does not have effect on the “tension to failure” of the normal Achilles tendon in the adult male rat. Vogel 38 showed an increase in the tensile strength of tendons after corticosteroid administration. However, the repetition of the injections progressively weakened the tendons. Oxlund found rat tendons to be stronger and stiffer after 24 and 55 days of the steroid treatment. He suggested this was due to steroid action on the elastic component and that the viscous properties remained unchanged, an opionion in agreement with Vogels findings. Vargas & Ross investigated the effects of intravenous and peroral corticosteroid in two groups of patients undergoing ACL repair. The corticosteroid treated group were compared to a group who received similar surgical and medical therapy but no steroids. The corticosteroid treated group used 50% less analgesics, had a length of stay 59% less long and ambulated 38% more quickly than the control group. No differences were noted between groups in incidence of postoperative problems in a one year follow-up. Wrenn published an experimental study showing a decrease in the tensile strength of tendons after corticosteroid therapy. He showed with dogs that the daily administration of 10 mg/kg of bodyweight intramuscular cortisone inhibited excessive formation of peritendinous fibrous tissue, but on the other hand also reduced the breaking point of the sutured tendons compared with the control group. It should be noted that the dose of corticosteroid used far exceed the relative doses (mg/kg bodyweight) used in humans. Concerning the histological changes after corticosteroid injections, Guttu evaluated the changes that occur in rat skeletal muscle injected with local anaesthetic and steroid. Rats injected with saline, steroid or procaine showed minimal reaction. Rats injected with the procaine and steroid combination had focal areas of inflammation at twenty-four hours but none on subsequent evaluations. The bupivacaine injected rats showed moderate localized necrosis of muscle fibres for less than tree weeks. The rats injected with the bupivacaine and steroid combination showed extensive localized necrosis of muscle fibres for more than four weeks. He concluded that steroids injected intramuscularly do no harm, but when it is injected in combination with bupivacaine it increases the tissue damage of bupivacaine and prolongs the healing phase. In very large series of histological examinations of spontaneously ruptured tendons steroid-induced lesions were very rare giving evidence that steroid-induced tendon ruptures are not a major problem in a population rupturing their tendons. In conclusion, it is documented that corticosteroid injection can indeed reduce the inflammatory process. It is well known that patients with inflammatory diseases have spontaneous tendon ruptures, and tendon ruptures are the end stage of many chronic sports injuries (Jumper s knee, Achilles tendinitis). Post mortem studies indicate that degenerative changes in tendons are part of a normal aging process. Most animal studies indicate that intratendinous injection of corticosteroid results in collagen necrosis of the tendon. No studies indicate the same risk in peritendinous injection of corticosteroid. Despite the large use of corticosteroid injection, prospective, randomised studies are lacking. Other possible adverse effects of corticosteroids. Introducing an infection is a possible adverse effect when using local steroid injection therapy. Not only the millions of tiny corticosteroid micro-crystals physically protect bacteria from the body defence, but also the local immune inflammatory response to infections is suppressed by the antiinflammatory action of the corticosteroid itself. However, this risk can be virtually completely eliminated by a meticulous aseptic, no-touch technique, and by avoiding injections in areas with suspected infection. Atrophy of the overlying skin with telangiectasia and increased hyperesthesia or hypoesthesia, and transparency can be caused if some injected material may leak back along the needle track. This seems to do little harm and recedes with time 49?51. Subcutaneous fat necrosis is also described following corticosteroid injections. Systemic effect of the corticosteroid is a possible risk. Although locally injected corticosteroids are designed to be most effective where they are injected, a proportion of the substance penetrates to the blood stream, especially if injections are repeated too frequently, and may cause adrenal cortical suppression, depression of osteoblastic activity or hypoglycemia. The latter can be dangerous for diabetic patients, as is the case with hyperglycemia. Signs of inflammation, causing concerns of possible secondary infection can occasionally be seen after corticosteroid injection. This inflammatory and irritation response can be treated with NSAID and cold compresses. It is usually transient and disappears within 24 hours. Penetration of minor blood vessels or nerves causing hematoma or sensibility disturbances is, as in any other injections, a possibility, too. Certainly, if the doctor that performs the injection is inexperienced, unintentional damage to other structures is possible. Corticosteroid injected into larger nerves can cause postinjection neuritis. The risk of this complication is negligible if the doctor is familiar with the ease by which the injection should be done. A sudden paresthesia suggests instantaneously end of the injection. Anaphylactic shock is a theoretical complication, which doctors must be prepared to treat since cortison allergy is a rare but possible form of allergy. A much more common injection-induced problem is the transient faintness of the patient, but this has nothing to do with corticosteroids as a substance. Progressive degenerative arthritis following intraarticular steroid injection was found by Chandler. Despite such reports, evidence for steroid arthropathy remains anecdotal, with scattered case reports, and confused by variables such as antecedent trauma or gross ligamentous instability. However, in 1991 and 1995 Pelletier called this observation in question. Pelletier examined the effect of intraarticular injections of corticosteroid in the knees of dogs in which the anterior cruciate ligament had been sectioned. Four groups were used: group one had one injection at 8 week, group two had two injections at 4 and 8 weeks, group three had tree injections at time of surgery and at 4 and 8 weeks, and group four had no injections. Injections with corticosteroid significantly reduced the size of osteophytes in group three (p0.0001) and group two (p0.0002). He concluded that corticosteroid injections on osteoarthritis cartilage lesions not only had a protective effect but also a therapeutic effect. The progressive degenerative arthritis following intraarticular steroid injection as found by Chandler could be due to accidental injections into the articular cartilage. This could explain the controversy between the results of Chandler and Pelletier. Inflammation itself makes necrosis of the joint surfaces. Aseptic necrosis of the joint surface due to infraction of the subchondrale bone is known to occur in joints in patients with severe rheumatoid arthritis who have never had corticosteroid therapy. Balch found in 65 knees that gross deterioration did not correlate with the number of injections but rather with the activity of the subject and the underlying disease process. The clinical anti-inflammatory effect of corticosteroid injections. Many authors have recorded favourable results after local steroid injections. Some authors did not found local steroid to have effect on the outcome. However, there are very few prospective, randomized studies: White found essentially no differences in the short term efficacy of oral indomethacine therapy compared to local corticosteroid injection(s) in the treatment of 40 patients with acute rotator cuff tendinitis. DaCruz examinated 28 patients with clinical Achilles paratendonitis and concluded that peritendinous injection of methyl prednisolone acetate is of no value. Smith found in 42 patients with nonseptic olecranon bursitis intrabursal injection of methylprednisolone acetate to be the most effective treatment regimen compared with oral naproxen and placebo. Girlanda 6,7 found a clear-cut efficacy of steroid injection therapy for carpal tunnel syndrome compared with placebo. In the treatment of trigger finger, Lambert 7 has shown a 60% success rate in a group receiving steroid injection against 16% for the control group receiving local anaesthetic (P 0,05), and, in treatment of tennis elbow, Price found the response of steroid injection significant better than for lignocaine. Relapses were common and at 24 weeks, the degrees of improvement were similar for the groups. In conclusion, there are only a few prospective, randomized studies concerning non-sports-induced inflammatory diseases. There have been no prospective randomized studies concerning the most common sports disorders, such as the Jumper s knee, Achilles tendinitis and tendinitis of the adductors in the groin. Preparation, doses and number of injections of corticosteroids and the clinical effect. The literature on comparative efficacy between different preparations, doses and number of injections is scanty: Price concluded in a double blind study that more rapid relief of symptoms of tennis elbow was achieved with 10 mg triamcinolone than with 25 mg hydrocortisone and there was less need to repeat injections in the former group, and Vogel 38 showed an increase in the tensile strength of tendons after corticosteroid injections, but repetition of injections progressively weakened the tendons, suggesting a relationship between cumulative dose and the adverse effect. Injections repeated too frequently can possible give systemic adverse effects. Discussion. Many investigators have reported case examples of tendon ruptures, especially among athletes, from injections of corticosteroid. The question remains whether these ruptures are the effect of steroids or merely a final manifestation of the disease for which the steroids were applied. When Hamilton 91 and many other authors state that steroids should never be used even around the tendon it appears to be the reiteration of an old dogma, and their writings do not present evidence to support this claim. All human studies are indeed anecdotal. There are no controlled trials and most cases involve chronic tendon lesions and lesions in patients with chronic inflammatory diseases, conditions with well-known high risks for spontaneous tendon ruptures even without steroid injections. The following criticism is indicative of the lack scientic evidence between corticosteroid injection and tendon rupture: Stannard reviewed the literature of triceps tendon ruptures and reported “the first case of triceps rupture associated with local steroid injections” used to treat an olecranon bursitis. In the same paper he reported one previous triceps rupture associated with olecranon bursitis in a patient who did not receive any steroid injections. Thus his rupture could be the result of the olecranon bursitis due to the pressure or the inflammation only. Alexeeff reported a case of rupture of the patella tendon in a young athlete with symptoms of “Jumpers knee” in one year. He had two corticosteroid injections that settled the symptoms and he resumed his normal training activities. Two years later he had a complete rupture. The relationship between the injections and the rupture remained unproven. In Subotnicks study, two of the 54 patients treated with steroids ruptured their tendons (3,7%) and he for this reason stated “… therefore steroids are not used.” However, in the same paper 10 ruptures in 284 (3,5%) no-steroid treated patients are presented. d’Anglejan concluded that the deterioration and ruptures of tendons seem favoured by local or general cortisone treatment, particularly among sportsmen. He based the conclusion on three patients suffering from chronic inflammatory disease, two cases of old people (84 years and 69 years) and the animal study of Ferland 28. Unverferth concluded in his study that all steroid injections are to be abandoned because local injection of steroid in and around the tendon predisposes it to complete rupture. However there were no arguments in his study allowing this conclusion. Some authors have published cases with bilateral tendon rupture in patients who had received corticosteroid injections. Because bilateral tendon rupture is an unusual occurrence, the authors concluded that the tendon rupture is a complication of corticosteroid injection. However, others have published cases with bilateral spontaneous tendon ruptures without concomitant systemic disease or steroid use. Kleinman and Gross reported Achilles tendon ruptures in three patients within six weeks of their receiving a single local steroid injection each. On the basis of rounding of the tendon ends and preexisting degenerative changes at the time of surgery repair, they concluded that it was not likely that the ruptures reflected a mere progression of existing tendinitis. It is not clear why the degenerative changes were ascribed to the effects of injection rather than other forms of microtrauma. However, many other such anecdotal reports are typical for the literature. Many of the conclusions are based on experiences from animal studies. However, human and animal fibroblasts can respond differently to steroids, suggesting that extrapolation of animal experiments to human must be interpreted with caution. Although it has been shown that intratendinous injection of corticosteroid has a directly deleterious effect on the tendon and should be unanimously condemned, there exists no reliable proof of deleterious effects of peritendinous injections. Too many conclusions are, as shown, based on poor scientific evidence. No studies are found reporting the rate of rupture when no steroid treatments on tendons is used. Spontaneous tendon ruptures have not undergone controlled studies. Thus, no comparison can be made between the incidences of spontaneous rupture (that obviously exists) and that of the steroid-induced ruptures, and it may well be that there is no difference. Leadbetter emphasize that because of the potential risks corticosteroid injections for treatment of acute and chronic sports injuries should be used with caution, but until more biologically selective drugs become available, the judicious application of local corticosteroid therapy remains a useful, albeit adjunctive therapy for sports injury. Buckwalter and Woo concluded in their recent review that the efficacy of steroidal anti-inflammatory drugs in minimizing tissue damage and accelerating a return to normal function after injury have not been proved in controlled studies, and the physicians treating patients with sports injuries should understand the potential adverse effect as well as the potential benefits of corticosteroid injections. Mahler in turn, concluded in his review that it does not seem reasonable to condemn peritendinous injection by invoking a direct deleterious effect on the tendon itself. Another interesting issue is how many times a same structure can be injected. The rules to be followed are empirical ones, guided more by common sense and experience than by systematic studies. If a local injection does not work first time, it may be reasonable to repeat it once – the first one may not have been placed accurately. If injection fails a second time, it is not wise to try again. Injections that are becoming too regular mean that the technique has not proved successful and other therapies should be sought. Perhaps the greatest criticism that can be raised regarding corticosteroid treatment as a sole solution in sports injury is that it tends, in its worst application, to be too passive and depend a modality and does not challenge the athlete s sense of responsibility to proper training, conditioning, and for developing correct technique. Improper diagnoses are an important fact that has lead to the controversy on the effect on corticosteroid injection. In Shields and Ljungqvist s studies on ruptures of the Achilles tendon, 25%-33% of the patients were given corticosteroid injections after an acute rupture. This high frequency is surprising, because erroneous intratendinous injections in humans are very painful, but in partial ruptured or degenerated tendons the resistance of the needle is probably not felt properly. According to current unkowledge, it is clear that corticosteroid injections have no place after an acute complete or partial rupture or in focal tendon degeneration, and partial tendon ruptures and degenerative focuses should be excluded (if necessary by ultrasound or MRI) before injection of corticosteroid. The improvement of ultrasound and MRI devices has made radiologic examinations an important tool when diagnosing and treating soft tissue injuries in sports medicine. In estimating tendons in patients with sport injuries, ultrasound and MRI of soft tissue lesions have offered morphologic information that is often unattainable by clinical judgement only. New power Doppler sonography will further improve the diagnostic accuracy of ultrasound revealing if hyperperfusion is associated with musculoskeletal inflammatory lesions. It may become an indispensable tool when establishing the diagnosis (inflammation or focal degeneration) before local steroid injection and controlling the effect of the injection treatment. Based on the above, the following safeguards of the table I should be followed when conducting local injection therapy with corticosteroids. Table 1. An appropriate use of corticosteroid-anaesthetic injections in sport. Modified with permission from Jozsa & Kannus. (Reviewed 2001 by U.Fredberg)
For references see Fredberg, U. Local corticosteroid injection in sport: review of literature and guidelines for treatment. Scand Jour Med Sci Sports 1997:7 (3):131-139 |
Treatment(1)
|
Local corticosteroid injection in sport: review of literature and guidelines for treatment. |
Examination
|
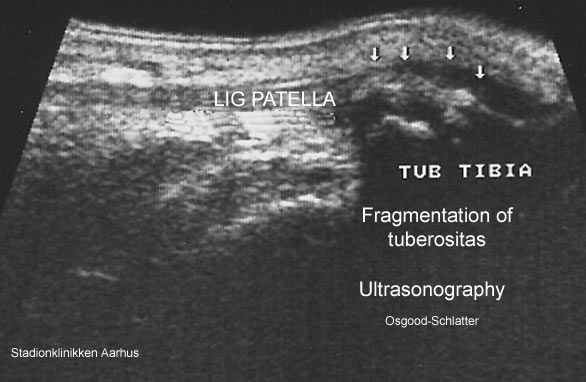
Ultrasonographic findings in Osgood-Schlatter disease. |

Examination(Ultrasonic image)
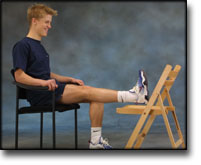
STEP2
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR OSGOOD-SCHLATTER
(OSGOOD-SCHLATTER)
STEP 2 |
|
|||||||||||||||||||||








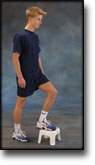
STEP3
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR OSGOOD-SCHLATTER
(OSGOOD-SCHLATTER)
STEP 3 |
|
||||||||||||||||||||||

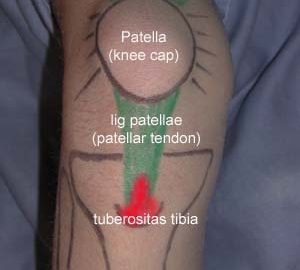
Anatomy(PHOTO)

STEP1
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR OSGOOD-SCHLATTER
(OSGOOD-SCHLATTER)
STEP 1 |
|
|||||||||||||||
STEP4
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR OSGOOD-SCHLATTER
(OSGOOD-SCHLATTER)
STEP 4 |
|
|||||||||||||||||||

