|
Results of non-operative and operative treatment of humeral shaft fractures. A series of 104 cases. |
Kategoriarkiv: Shoulder
treatment-article
|
Complications of plate fixation in fresh displaced midclavicular fractures. METHODS. RESULTS. CONCLUSIONS. |
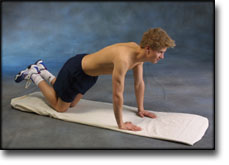
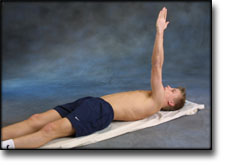
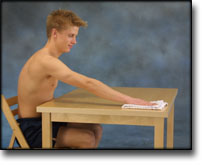
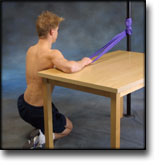
step4
Training ladder for:
FROZEN SHOULDER
(PERIARTROSIS HUMEROSCAPULARIS)
STEP 4 |
|
|||||||||||||||||||||||||||||||||||||||||||||||









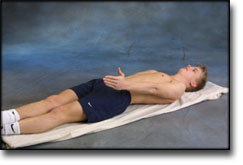












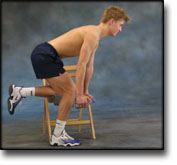
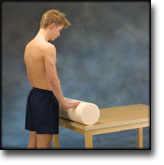
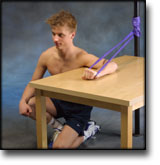
step3
Training ladder for:
FROZEN SHOULDER
(PERIARTROSIS HUMEROSCAPULARIS)
STEP 3 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



















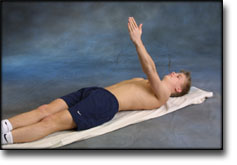
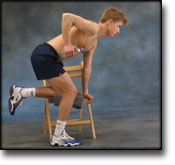
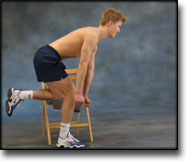
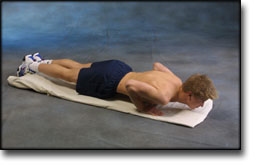
step2
Training ladder for:
FROZEN SHOULDER
(PERIARTROSIS HUMEROSCAPULARIS)
STEP 2 |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

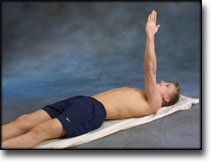












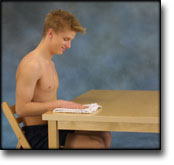




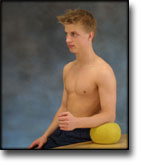
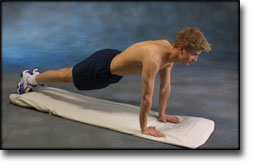
step1
Training ladder for:
FROZEN SHOULDER
(PERIARTROSIS HUMEROSCAPULARIS)
STEP 1 |
|
||||||||||||||||||||||||||||||||||||||||||||








treatment-article2
|
Frozen shoulder: a 12-month clinical outcome trial. |
treatment-article1
|
Intra-articular triamcinolone acetonide injection in patients with capsulitis of the shoulder: a comparative study of two dose regimens. SUBJECTS. METHOD. RESULTS. CONCLUSIONS. |
symptoms-article
|
Humero-scapular periarthrosis. |
step4
Training ladder for:
MUSCLE INFILTRATIONS IN THE NECK-SHOULDER
(MYOSER)
STEP 4 |
Unlimited: Cycling. Swimming. Running.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |