|
Efficacy of thigh protectors in preventing thigh haematomas. |
Kategoriarkiv: Thigh, front
treatment-article2
|
Acute compartment syndrome. |
treatment-article1
|
Thigh compartment syndrome in a football athlete: a case report and review of the literature. |
step4
Training ladder for:
CHRONIC COMPARTMENT SYNDROME IN THE ANTERIOR THIGH
(CHRONIC KOMPARTMENT SYNDROM)
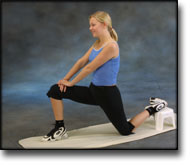
STEP 4 |
Unlimited: Cycling. Swimming. Running and spurting.
|
||||||||||||||||||||||||||||||||||||||||||||||||





















|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step3
Training ladder for:
CHRONIC COMPARTMENT SYNDROME IN THE ANTERIOR THIGH
(CHRONIC KOMPARTMENT SYNDROM)
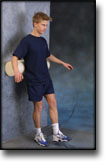
STEP 3 |
Unlimited: Cycling. Swimming. Light running./SPAN>
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step2
Training ladder for:
CHRONIC COMPARTMENT SYNDROME IN THE ANTERIOR THIGH
(CHRONIC KOMPARTMENT SYNDROM)
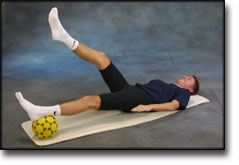
STEP 2 |
Unlimited: Cycling. Swimming. Jogging.
|
||||||||||||||||||||||||||||||||||||||||||||

|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step1
Training ladder for:
CHRONIC COMPARTMENT SYNDROME IN THE ANTERIOR THIGH
(CHRONIC KOMPARTMENT SYNDROM)
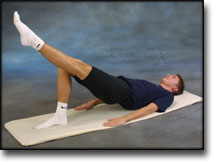
STEP 1 |
| The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
|
||||||||||||||||||||||||||||||||||||||||||||||




|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
treatment-article2
|
Good results of fasciotomy in chronic compartment syndrome of the lower leg. DESIGN. SETTING. METHOD. RESULTS. CONCLUSION. |
treatment-article1
|
Chronic compartment syndrome of the quadriceps femoris muscle in athletes. Diagnosis, imaging and treatment with fasciotomy. MATERIAL AND METHODS. RESULTS AND CONCLUSIONS. |
treatment-article
|
Treatment of chronic exertional anterior compartment syndrome with massage: a pilot study. DESIGN. SETTING. PARTICIPANTS. INTERVENTIONS. MAIN OUTCOME MEASURES. RESULTS. CONCLUSIONS. |