|
Femoral stress fractures in children. |
|
Fractures of the femoral neck in children: complications and their treatment |
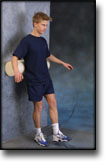
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR MUSCULAR BLEEDING IN THE ANTERIOR THIGH
(HAEMATOMA MUSCULI)
STEP 4 |
| The following rehabilitation program will cover the needs for the vast majority of children with muscle bleeding in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults. | |||||||||||||||||||||||||||
| Unlimited: Cycling. Swimming. Running with jumping.
|
|||||||||||||||||||||||||||
| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR MUSCULAR BLEEDING IN THE ANTERIOR THIGH
(HAEMATOMA MUSCULI)
STEP 3 |
| The following rehabilitation program will cover the needs for the vast majority of children with muscle bleeding in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults. | |||||||||||||||||||||
| Unlimited: Cycling. Swimming. Running with increasing distance.
|
|||||||||||||||||||||
| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
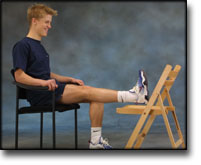
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR MUSCULAR BLEEDING IN THE ANTERIOR THIGH
(HAEMATOMA MUSCULI)
STEP 2 |
| The following rehabilitation program will cover the needs for the vast majority of children with muscle bleeding in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults. | ||||||||||||||||||
| Unlimited: Cycling with a weak load. Swimming. Jogging.
|
||||||||||||||||||
| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR MUSCULAR BLEEDING IN THE ANTERIOR THIGH
(HAEMATOMA MUSCULI)
STEP 1 |
| The following rehabilitation program will cover the needs for the vast majority of children with muscle bleeding in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults. | ||||||||||||||
| Unlimited: Cycling with a weak load. Swimming.
|
||||||||||||||
| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
|
The painless soft tissue mass in childhood–tumour or not? |
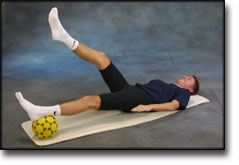
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR MUSCLE RUPTURE IN THE POSTERIOR THIGH
(RUPTURA MUSCULI)
STEP 4 |
|
|||||||||||||||||||
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR MUSCLE RUPTURE IN THE POSTERIOR THIGH
(RUPTURA MUSCULI)
STEP 3 |
|
|||||||||||||||||||||