|
||
|
||
|
||
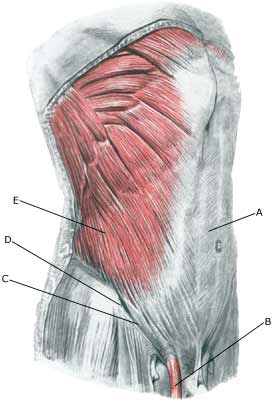
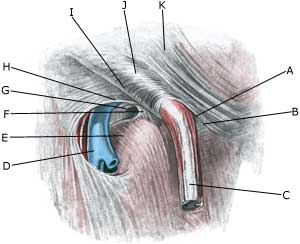
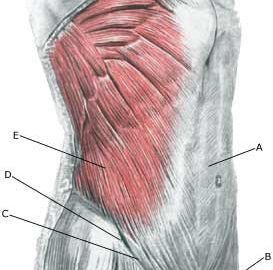
| Cause: If the abdominal wall becomes too weak, the intestines can be pressed through the weak spots in the abdominal wall causing a hernia.
Symptoms: Pain in the groin, aggravated when coughing. Sometimes a swelling in the groin is visible. Usually the swelling (containing intestine) can be pushed into place. If the swelling is painful and cannot be pressed into place the hernia may be strangulated (which requires acute medical assistance). Examination: In obvious cases with visible swelling in the groin the diagnosis is easy to make. With lack of swelling in the groin the diagnosis is naturally difficult. (article 1) A normal medical examination is usually sufficient in order to make the diagnosis, however, if there is any doubt concerning the diagnosis a MRI-scan or a dynamic ultrasound scan, where weaknesses in the abdominal wall can be detected while increasing the pressure in the abdominal cavity by applying pressure can be performed (article 2) (article 3). Treatment: With modest discomfort, you can primarily attempt training of the abdominal muscles (article). If discomfort continues, surgery is advised. If strangulated hernia is suspected you should seek acute medical assistance to evaluate the indication for acute surgery, as there is a risk of lasting damage to the intestine. With uncomplicated surgery, a relief period of approx. two months should be expected before maximal sports activity can be resumed (very dependent on the sport in question). Complications: If progress is not smooth (even after operation) it should be considered whether the diagnosis is correct or whether complication have arisen. In particular the following should be considered:
|