|
||
|
||
|
||
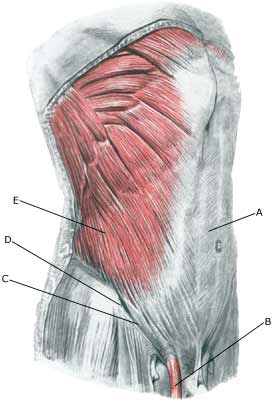
| Cause: The existence of “sportsman’s hernia” is debated amongst professionals (article 1). Generally it involves a inguinal hernia (direct hernia), that can not be detected with certainty neither before nor after surgery. Some consider the condition to be an early stage of an imminent inguinal hernia, while others believe it to be small ruptures in the muscles and tendons around the inguinal canal (article 2) (article 3).
Symptoms: Pain in the groin without any detectable swelling in the groin or any other explanation for the pain. Examination: There are no examinations (X-ray, ultrasound, MRI-scan, scintigraphy), that can detect the sportsman’s hernia (article). Previously used attempts with X-ray contrast in the abdominal cavity (herniography) showed “sportsman’s hernia” in 49% of healthy subjects, which naturally renders the examination unusable. Treatment: Before you choose to be operated for “sportsman’s hernia”, all non-operative possibilities should be attempted, including sufficient relief and rehabilitation of the most tender structures and muscles. Training of the muscles around the groin, stomach and loin before possible surgery. Complications: Since it may be difficult to make a correct diagnosis in athletes with long-term groin pain (article). A multidisciplinary approach, it should be supplemented with, amongst other things, ultrasound scan and consideration of X-ray scintigraphy and possibly MRI-scan. You should of course consider the correctness of the diagnosis and amongst other things consider the following:
|