|
US of the snapping iliopsoas tendon. MATERIALS AND METHODS. RESULTS. CONCLUSION. |
Alle indlæg af urtehave_com
examination-article1
|
The snapping hip: clinical and imaging findings in transient subluxation of the iliopsoas tendon. PATIENTS AND METHODS. RESULTS. CONCLUSIONS. |
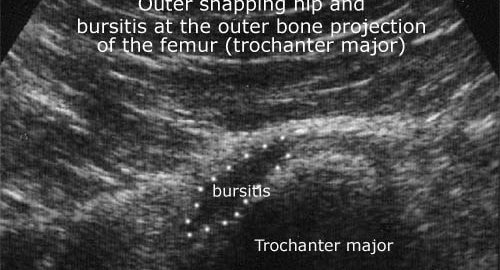
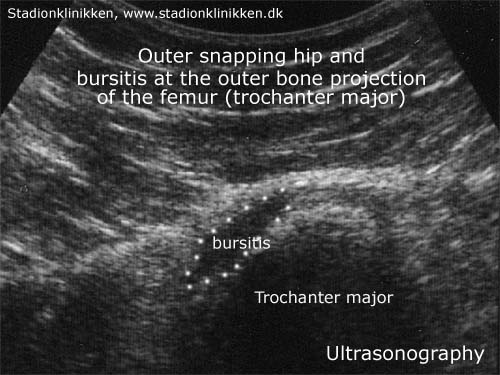
bursitis
Cause: In case of repeated loads or blows, the bursa can produce additional fluid, swell and become inflamed and painful. Symptoms: Pain when applying pressure on the bursa, which sometimes (but far from always) can feel swollen. Pain is aggravated upon activation of the muscle closest to the bursa. Acute treatment: Click here. Examination: In light cases with only minimal tenderness, medical examination is not necessarily required. In case of more pronounced pain or lack of progress, a medical examination should be carried out to ensure the correctness of the diagnosis and the commencement of any treatment. The diagnosis is most easily and quickly made with ultrasound (which allows simultaneous treatment). Treatment: The treatment primarily comprises relief. If the direct cause of the complaint is known, it should of course be removed. The treatment can be supplemented by rheumatic medicine (NSAID) or injection of corticosteroid in the bursa, preceded by draining of this, which can advantageously be performed under ultrasound guidance. Rehabilitation: The treatment is dependant upon which bursa is inflamed, but sports activity can usually be cautiously resumed when pain has diminished, especially if the provoking factor has been identified and removed. Complications: If progress is not smooth, the correctness of the diagnosis or whether complications have arisen should be considered:
Special: Shock absorbing shoes or inlays will reduce the load. |
step4
Training ladder for:
OUTER SNAPPING HIP
(COXA SALTANS, EXTERN)
STEP 4 |
Unlimited: Cycling. Swimming. Running.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||























|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step3
Training ladder for:
OUTER SNAPPING HIP
(COXA SALTANS, EXTERN)
STEP 3 |
Unlimited: Cycling with raised saddle. Swimming. Running with increasing speed and distance.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||









|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step2
Training ladder for:
OUTER SNAPPING HIP
(COXA SALTANS, EXTERN)
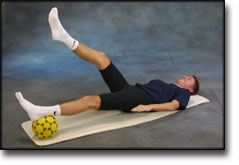
STEP 2 |
Unlimited: Cycling with raised saddle. Swimming. Light jogging.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||





|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
step1
Training ladder for:
OUTER SNAPPING HIP
(COXA SALTANS, EXTERN)
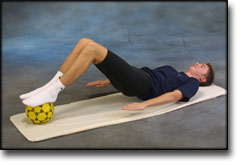
STEP 1 |
| The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
examination-article
|
Extraarticular snapping hip: sonographic findings. MATERIALS AND METHODS. RESULTS. CONCLUSION. |
ultrasonic-image
cause-article
|
Coxa Saltans: The Snapping Hip Revisited. |