Untitled Document
|
||
|
||
|
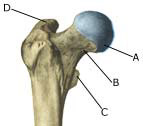
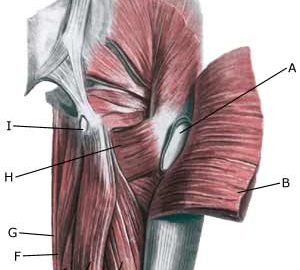
Cause: Inflammation of the tendon fastenings (tendinitis) at the ischiatic bone (tuber ischiadicum) occurs following repeated uniform (over)loads (e.g. running, sprinting) causing microscopic ruptures in the tendon, and especially at the tendon fastening in the growth zone. Inflammation is a warning that the training performed is too strenuous for the muscles in question. In some cases, a single strenuous load can cause a piece of the ischiatic bone to be torn off in the growth zone (article).
Symptoms: Pain in the growth zone in the ischiatic bone can occasionally radiate down into the rear of the thigh. The pain is aggravated when applying pressure on the bone (e.g. sitting position), stretching and activating the posterior thigh muscles (flexing the knee against resistance). Examination: In slight cases with only minimal tenderness and no discomfort with walking, medical examination is not necessarily required. The extent of the tenderness is, however, not always a mark of the degree of the injury. In cases of more pronounced pain or tenderness, medical examination is required to ensure the correct diagnosis and treatment. The diagnosis is usually made on the basis of a normal medical examination, however, if there is any doubt concerning the diagnosis, this can be confirmed by ultrasound scanning or MR scanning (article). X-ray can be considered if sudden powerful pain is experienced, as this could indicate suspicions of a bone tear. Treatment: The treatment usually comprises relief, stretching and rehabilitation (article). It can be necessary to re-join the piece of the ischiatic bone which has torn off in the growth zone under surgery in some cases, however, many cases can be successfully treated with relief (article). Complications: If the treatment does not progress according to plan, it should be considered if the diagnosis is correct or whether complications have arisen. The following should in particular be considered:
Special: Adolescents nearing the end of their teenage years should refer to the adult SportNetDoc under tendonitis at the ischiatic bone. |