Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 4
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Cycling. Running. Swimming.
(10 min)
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
Stand and bounce a ball on the floor backwards and forwards from the injured to the good hand.
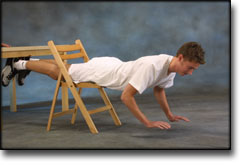
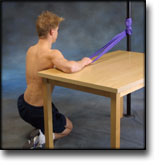
Lie on your stomach across a chair with both feet supported under a tabletop. Lift both hands from the floor and hold the position for 2 seconds. Support with your hands for 2 seconds and repeat the exercise 10 times in quick succession.
Support with both hands against a wall. Move slowly towards the wall and push away again. The exercise is performed like standing push-ups.
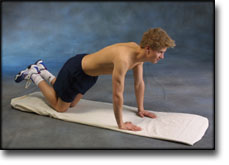
Go down on all fours. Lift your toes from the floor and do push-ups.
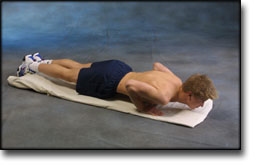
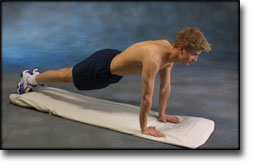
Lie on the floor with instep stretched. Support on your toes and do push-ups without your stomach touching the floor.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 3
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Cycling. Running. Swimming.
(10 min)
Rotate the forearm so that the palm faces alternately up and down.
Bend and stretch the arm to the extreme position. Cautiously apply pressure in the extreme position to achieve maximum mobility.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 2
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Running. Cycling.
(20 min – Primarily to achieve full mobility)
Rotate the forearm so that the palm faces alternately up and down.
Bend and stretch the arm to the extreme position. Cautiously apply pressure in the extreme position to achieve maximum mobility.
(40 min)
Stand holding a firm round cushion against the wall with the injured arm. Slowly move the cushion up the wall above 90 degrees.
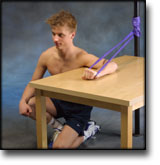
Lie on your stomach across a table or chair and support with both arms on the floor. Raise one arm from the floor and hold the position for approx. 10 seconds. Change arm.
Lie on your back with support at the elbow. Slowly bend and stretch the elbow while holding a weight.
Lie on your stomach on a bench or table with the injured arm hanging over the edge holding a weight or bottle. Slowly draw the hand up to the shoulder joint.
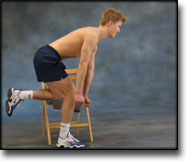
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. You can bend your arm if you have difficulty in locating the shoulder blade muscles.
Sit at a table holding a hammer in the injured hand, with the arm resting on the table and the hand over the edge. Slowly rotate the lower arm from side to side.
Using an elastic band around the back of the injured hand, move the wrist upwards while keeping the elastic taut.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 1
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Running.
(20 min – Primarily to achieve full mobility)
Rotate the forearm so that the palm faces alternately up and down.
Bend and stretch the arm to the extreme position. Cautiously apply pressure in the extreme position to achieve maximum mobility.
(40 min)
Squeeze a soft ball.
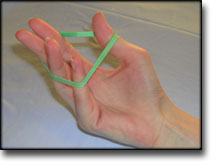
Put an elastic band around your fingers. Spread your fingers so that the elastic is stretched.
Stand at a table with the injured arm on a ball. Move the ball in all directions while applying slight pressure on the ball.
Let the injured hand hang over the edge of a table with the palm facing downwards. Move the hand slowly up and down while holding a weight. Support the injured arm with the good arm.
Sit at a table with the injured hand on a ball and roll slowly from side to side.
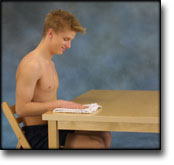
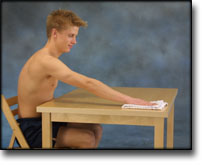
Sit with the injured arm on a table with your hand on a cloth. Polish the tabletop backwards and forwards while applying slight pressure with your arm.
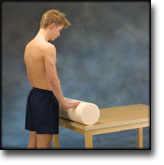
Stand at a table with both hands on a firm round cushion with elbows slightly bent. Apply slight pressure to the cushion and roll the cushion away from yourself so that the upper body bends in over the table. Roll the cushion back again to the starting position.
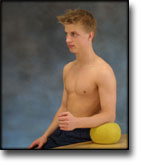
Sit at a table with the injured arm’s elbow on a ball. Press against the ball with a slow movement for 5 seconds. Rest for 5 seconds before repeating.
Sit at a table with the injured hand on a ball and roll slowly backwards and forwards.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Walter E, Holz U, Kohle H. Orthopade 1988 Jun;17(3):306-12
This paper briefly presents the anatomy of the elbow joint, its pathophysiology, the various types of dislocation of the elbow joint and concomitant injuries, the appropriate diagnostic procedures and the indications for surgery and the operative technique applied for correction of dislocation. The only urgent indications for operative treatment are elbow joint dislocation with concomitant bone injuries, persistent instability or luxation position, open injuries and vessel and/or nerve injuries. For purely ligamentous lesions combined with relative loss of stability an operative procedure does not seem necessary. The operative technique applied for the treatment of habitual or recurrent dislocation is also described.
Return to Australian rules football after acute elbow dislocation: A report of three cases and review of the literature.
Verrall GM. J Sci Med Sport 2001 Jun;4(2):245-50
Acute elbow dislocation is an uncommon problem encountered in contact sports such as Australian Rules Football [ARF]. Previously there have been few guidelines presented as to when the athlete can safely return to sport following such an injury. During the 1998 playing season the author as medical officer of a professional ARF team encountered three athletes who had an elbow dislocation. All resulted from a fall on an outstretched hand during competition. The athletes returned to football at 13 days, 21 days and 7 days respectively. All subsequently completed the football season without re-injury and at post-season clinical review and one year subsequent to this no athlete described residual symptoms nor was there any loss of range of motion of the elbow joint. Clinical recommendations that allow for athletes to make a safe and early return to contact sport following an episode of acute elbow dislocation include; 1) commencing active mobilization as soon as possible after injury, 2) using passive mobilization to attain full extension as soon as possible, 3) allowing the athlete to return to training before full extension is achieved and 4) allowing the athlete to return to contact sport as soon as full extension is achieved with assistance of elbow stability taping.
Acute elbow dislocation: evaluation and management.
Cohen MS, Hastings H 2nd. J Am Acad Orthop Surg 1998 Jan-Feb;6(1):15-23
Most elbow dislocations are stable after closed reduction. Treatment with an early range-of-motion program generally leads to favorable results. Care must be taken to rule out neurovascular involvement and associated osseous or ligamentous injury in the wrist. Late elbow instability and stiffness are rare after simple dislocations. Complex elbow dislocations with associated fractures may require surgical intervention to obtain joint stability; ligament and/or fracture repair is frequently necessary in this situation. Larger periarticular fractures adversely affect functional results. Potential late complications of elbow dislocation include posttraumatic stiffness, posterolateral joint instability, ectopic ossification, and occult distal radioulnar joint disruption.