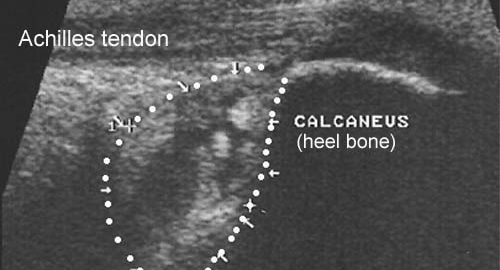
Training ladder for: SLIMSÆKSBETÆNDELSE VED ACHILLESSENEFÆSTET (BURSITIS ACHILLES)
STEP 4
It is imperative to ensure that the shoes do not pinch the heel, and have a sound shock absorbing sole.
Unlimited: Cycling. Swimming. Running with increasing distance on a soft surface.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(45 min)
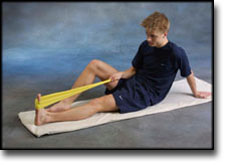
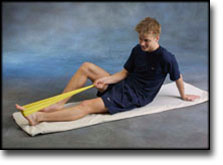
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand on a soft surface. Rise slowly up on tiptoe and go down again.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: SLIMSÆKSBETÆNDELSE VED ACHILLESSENEFÆSTET (BURSITIS ACHILLES)
STEP 3
It is imperative to ensure that the shoes do not pinch the heel, and have a sound shock absorbing sole.
Unlimited: Cycling. Swimming. Light jogging on a smooth surface.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(45 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand on a soft surface. Rise slowly up on tiptoe and go down again.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: SLIMSÆKSBETÆNDELSE VED ACHILLESSENEFÆSTET (BURSITIS ACHILLES)
STEP 2
It is imperative to ensure that the shoes do not pinch the heel, and have a sound shock absorbing sole.
Unlimited: Cycling. Swimming. Running in deep water.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(45 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand on a soft surface. Rise slowly up on tiptoe and go down again.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: SLIMSÆKSBETÆNDELSE VED ACHILLESSENEFÆSTET (BURSITIS ACHILLES)
STEP 1
It is imperative to ensure that the shoes do not pinch the heel, and have a sound shock absorbing sole.
The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
Unlimited: Cycling. Swimming.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(45 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Surgical management of Achilles tendon overuse injuries. A long-term follow-up study.
Schepsis AA, Wagner C, Leach RE. Am J Sports Med 1994 Sep-Oct;22(5):611-9.
We studied 79 cases of surgically treated Achilles tendon overuse injuries in 66 patients. Fifty-three (80%) of these patients were competitive or serious recreational runners operated on between 1978 and 1991. There were 49 men and 17 women with a mean age of 33 years (range, 17 to 59). The cases were divided into surgical subgroups based on their site of primary symptoms and abnormalities: paratenonitis (23), tendinosis (partial rupture or degeneration) (15), retrocalcaneal bursitis (24), insertional tendinitis (7), and combined abnormalities (10). Followup included a comprehensive patient questionnaire and office examination. There were 79% satisfactory (51% excellent, 28% good) and 21% unsatisfactory (17% fair, 4% poor) results. The percentages of satisfactory results in the paratenonitis group (87%) were best and those in the tendinosis group were the worst (67%). Satisfactory results were obtained in 75% of the patients with retrocalcaneal bursitis and 86% with insertional tendinitis. Seven of the 45 cases with longer than 5-year followup with initially satisfactory results deteriorated with time and required reoperation (16%). Of these, 4 were in the tendinosis group, 2 had retrocalcaneal bursitis, and 1 had paratenonitis. One of the 34 patients followed less than 5 years required reoperation.
Comparison of results of retrocalcaneal decompression for retrocalcaneal bursitis and insertional achilles tendinosis with calcific spur.
Watson AD, Anderson RB, Davis WH. Foot Ankle Int 2000 Aug;21(8):638-42.
Sixteen feet with retrocalcaneal bursitis (RB) and twenty-two feet with calcific Achilles insertional tendinosis (IAT-CS) underwent retrocalcaneal decompression after failure of nonoperative treatment. Follow-up evaluation at least two years after surgery included AOFAS Ankle-Hindfoot subscale scores, satisfaction, time until maximum symptomatic improvement, and radiographs. Statistically significant differences between the groups include the following: IAT-CS patients were older, required nearly twice the time to reach maximum symptomatic improvement, had lower satisfaction rates, had a lower pain score, and more frequently had shoewear restrictions. Radiographic recurrence did not correlate with outcome or symptomatic recurrence.