Training ladder for: RUPTURE OF THE ACHILLES TENDON (RUPTURA TRAUMATICA TENDINIS ACHILLES)
STEP 4
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Unlimited: Cycling. Swimming. Running with increasing distance on a soft surface.
(5 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Stand on the leg to be trained. Take-off and land on the same leg.
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(50 min)
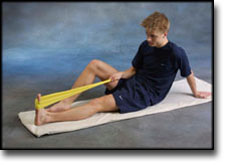
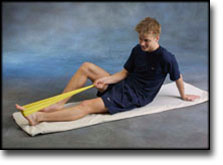
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand on a soft surface. Rise slowly up on tiptoe and go down again.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Stand with both forefeet on a stool or doorstep with the heel out over the edge. Slowly rise up on to your toes with your weight on the healthy leg. Go slowly down on the injured leg as far as you can go. Use the healthy leg to rise up on to your toes again. The exercise should be performed with stretched, as well as bent knee. Wearing a rucksack and gradually increasing the ballast in the rucksack can increase the load.
Stand with feet together. Using the ankle joint to take off, hop approx. 5 cm and land on both feet. The exercise should be done on one leg when you are able to do it without discomfort using both legs.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: RUPTURE OF THE ACHILLES TENDON (RUPTURA TRAUMATICA TENDINIS ACHILLES)
STEP 3
Unlimited: Cycling. Swimming. Light jogging on a smooth surface.
(5 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(50 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand on a soft surface. Rise slowly up on tiptoe and go down again.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Stand with both forefeet on a stool or doorstep with the heel out over the edge. Slowly rise up on to your toes with your weight on the healthy leg. Go slowly down on the injured leg as far as you can go. Use the healthy leg to rise up on to your toes again. The exercise should be performed with stretched, as well as bent knee. Wearing a rucksack and gradually increasing the ballast in the rucksack can increase the load.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: RUPTURE OF THE ACHILLES TENDON (RUPTURA TRAUMATICA TENDINIS ACHILLES)
STEP 2
Unlimited: Cycling. Swimming. Running in deep water.
(Ingen øvelser)
(5 min)
Stand on one leg. Play the ball up against the wall.
(55 min)
Lay on the floor with a cushion under the calf. Tip the foot up and down without putting any resistance on the foot.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: RUPTURE OF THE ACHILLES TENDON (RUPTURA TRAUMATICA TENDINIS ACHILLES)
STEP 1
The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
Unlimited: Cycling. Swimming.
(Ingen øvelser)
(5 min)
Stand on one leg on the floor or a mattress. Look straight ahead and keep the knee slightly bent.
(55 min)
Lay on the floor with a cushion under the calf. Tip the foot up and down without putting any resistance on the foot.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
An update on repair of Achilles tendon rupture. Acute and delayed.
Kuwada GT. J Am Podiatr Med Assoc 1999 Jun;89(6):302-6.
Current surgical treatments for Achilles tendon rupture are thoroughly discussed. New repair techniques, such as the use of soft-tissue anchors, are reviewed, as is the use of synthetic mesh to augment the surgical repair. A classification system devised by the author is presented to make it easier to select the appropriate surgical procedure or combination of procedures in delayed rupture repair. Postoperative physical therapy is paramount in the return to preinjury level of activity for these patients.
Diagnosis and treatment of acute ruptures of the Achilles tendon.
Current concepts review. Popovic N, Lemaire R. Acta Orthop Belg 1999 Dec;65(4):458-71.
Subcutaneous rupture of the Achilles tendon seems to have become more common in recent years. This results from a combination of more awareness in the medical field and greater participation in physical activities by the general population. The causes of Achilles tendon rupture are multifactorial and still unclear. The diagnosis can be made based on physical examination; special diagnostic studies are rarely necessary. The literature on ruptures of the Achilles tendon and associated treatment has expanded over the past decade. The lack of a universal, consistent protocol for subjective and objective evaluation following treatment of Achilles tendon rupture has prevented any comparison of results. There is still controversy concerning the best treatment. From a literature review, it appears that a satisfactory outcome may be achieved with either nonoperative or operative treatment but surgical repair appears to provide better functional capacity. Lower rerupture rates and slightly improved strength and functional ability may be expected with surgical treatment; however, the rate of minor complications is higher than with nonoperative treatment. Reports in the literature indicate that in active, young, very demanding individuals, surgical repair should be considered, with nonsurgical treatment reserved for elderly or sedentary patients. There is no single, uniformly accepted surgical technique for Achilles tendon repair. Most acute ruptures have been treated successfully with simple end-to-end suture, although various augmentation procedures have been combined with simple suture with satisfactory outcomes. To minimize the complications typically associated with open surgery, percutaneous techniques to repair the ruptured Achilles tendon have been advocated, and the results are reported to be promising, although not without failures and complications. Several recent studies have reported functional benefits of early postoperative tendon mobilization in well-motivated patients, since treatment results are determined not only by the method of repair but also, and perhaps more importantly, by the early postoperative functional rehabilitation.
Tendo Achillis rupture; surgical repair is a safe option.
Mellor SJ, Patterson MH. Injury 2000 Sep;31(7):489-91.
We reviewed the results of 67 tendo Achillis repairs performed at one District General Hospital over a 5-year period, using details from a comprehensive database. At a mean follow-up of 2.5 years, the re-rupture rate was 3% (2 out of 67). The infection rate was 1.5% (1 out of 67). A review of the relevant literature has revealed that quoted infection rates following tendo Achillis repair vary considerably, and are as high as 21%. Several authors have advised against repair based on those data. In the light of our results, we can recommend surgical repair of tendo Achillis rupture as a safe option.