TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR INFLAMMATION OF THE ACHILLES TENDON (TENDINITIS ACHILES)
STEP 4
The majority of young patients can manage with relief until the pain subsides, following which the sports activity can be slowly resumed. The following rehabilitation program will cover the needs for the vast majority of children with tendinitis at the Achilles tendon. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming. Running with increasing distance on a soft surface.
(15 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(10 min)
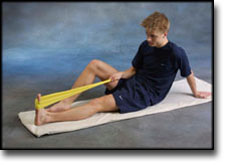
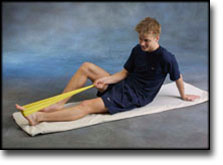
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand with both forefeet on a stool or doorstep with the heel out over the edge. Slowly rise up on to your toes with your weight on the healthy leg. Go slowly down on the injured leg as far as you can go. Use the healthy leg to rise up on to your toes again. The exercise should be performed with stretched, as well as bent knee. Wearing a rucksack and gradually increasing the ballast in the rucksack can increase the load.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR INFLAMMATION OF THE ACHILLES TENDON (TENDINITIS ACHILES)
STEP 3
The majority of young patients can manage with relief until the pain subsides, following which the sports activity can be slowly resumed. The following rehabilitation program will cover the needs for the vast majority of children with tendinitis at the Achilles tendon. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming. Light jogging (few minutes) on a soft surface.
(15 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand with both forefeet on a stool or doorstep with the heel out over the edge. Slowly rise up on to your toes with your weight on the healthy leg. Go slowly down on the injured leg as far as you can go. Use the healthy leg to rise up on to your toes again. The exercise should be performed with stretched, as well as bent knee. Wearing a rucksack and gradually increasing the ballast in the rucksack can increase the load.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR INFLAMMATION OF THE ACHILLES TENDON (TENDINITIS ACHILES)
STEP 2
The majority of young patients can manage with relief until the pain subsides, following which the sports activity can be slowly resumed. The following rehabilitation program will cover the needs for the vast majority of children with tendinitis at the Achilles tendon. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming.
(5 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand with both forefeet on a stool or doorstep with the heel out over the edge. Slowly rise up on to your toes with your weight on the healthy leg. Go slowly down on the injured leg as far as you can go. Use the healthy leg to rise up on to your toes again. The exercise should be performed with stretched, as well as bent knee. Wearing a rucksack and gradually increasing the ballast in the rucksack can increase the load.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR INFLAMMATION OF THE ACHILLES TENDON (TENDINITIS ACHILES)
STEP 1
The majority of young patients can manage with relief until the pain subsides, following which the sports activity can be slowly resumed. The following rehabilitation program will cover the needs for the vast majority of children with tendinitis at the Achilles tendon. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming.
(5 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(5 min)
Stand with both forefeet on a stool or doorstep with the heel out over the edge. Slowly rise up on to your toes with your weight on the healthy leg. Go slowly down on the injured leg as far as you can go. Use the healthy leg to rise up on to your toes again. The exercise should be performed with stretched, as well as bent knee. Wearing a rucksack and gradually increasing the ballast in the rucksack can increase the load.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Objective: Reduce the load on the Achilles tendon.
Application: The foot should be held slightly stretched while applying the tape (talipes equinus). Two tape “anchors” should be applied – one around the lower leg just below the knee, and one around the forefoot behind the toe pad (A). A strip of tape should be cut which is 10 cm longer than twice the distance between the two anchors. The strip should be folded in the middle and stuck together leaving it double thickness and only half as long. One end is taped on the back of the anchor below the knee, and the other end taped to the anchor under the sole (B). The ends of the strip are folded around the respective anchors, and are fixed with the help of a further anchor. The strip will then be able to act as a kind of “extra Achilles tendon” (C).
Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis.
Alfredson H, Pietila T, Jonsson P, Lorentzon R. Am J Sports Med 1998 May-Jun;26(3):360-6.
We prospectively studied the effect of heavy-load eccentric calf muscle training in 15 recreational athletes (12 men and 3 women; mean age, 44.3 +/- 7.0 years) who had the diagnosis of chronic Achilles tendinosis (degenerative changes) with a long duration of symptoms despite conventional nonsurgical treatment. Calf muscle strength and the amount of pain during activity (recorded on a visual analog scale) were measured before onset of training and after 12 weeks of eccentric training. At week 0, all patients had Achilles tendon pain not allowing running activity, and there was significantly lower eccentric and concentric calf muscle strength on the injured compared with the noninjured side. After the 12-week training period, all 15 patients were back at their preinjury levels with full running activity. There was a significant decrease in pain during activity, and the calf muscle strength on the injured side had increased significantly and did not differ significantly from that of the noninjured side. A comparison group of 15 recreational athletes with the same diagnosis and a long duration of symptoms had been treated conventionally, i.e., rest, nonsteroidal antiinflammatory drugs, changes of shoes or orthoses, physical therapy, and in all cases also with ordinary training programs. In no case was the conventional treatment successful, and all patients were ultimately treated surgically. Our treatment model with heavy-load eccentric calf muscle training has a very good short-term effect on athletes in their early forties.
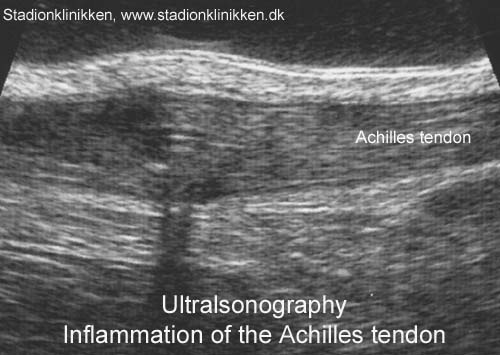
Ultrasonography in the differential diagnosis of Achilles tendon injuries and related disorders. A comparison between pre-operative ultrasonography and surgical findings.
Paavola M, Paakkala T, Kannus P, Jarvinen M. Acta Radiol 1998 Nov;39(6):612-9.
PURPOSE. To assess the value of US in the diagnosis of various Achilles tendon disorders.
MATERIAL AND METHODS. Pre-operative US was compared with surgical findings in 79 patients with an Achilles tendon complaint.
RESULTS. US was highly reliable for verifying a complete Achilles tendon rupture, only one false-negative US examination was found in the 26 surgically verified cases. For diagnosing retrocalcanear bursitis, US was accurate: 6 out of the 8 cases of bursitis were found and there were no false-positive cases. There were also no false-positive US findings in patients with peritendinitis/tendinitis, but 7 false-negative US cases among the 40 surgically verified peritendinitis/tendinitis patients indicated that a negative US finding in a clinically suspected case of peritendinitis/tendinitis is unreliable. US also seemed to be inadequate for differentiating partial tendon rupture from a focal tendon degeneration. Nevertheless, the occurrence and location of such a lesion could be adequately determined by US.
CONCLUSION. US can reliably be used for locating the Achilles tendon abnormality, estimating its severity, and determining most of the conditions requiring surgical intervention. However, US is not completely reliable for diagnosing peritendinitis and tendinitis, and it cannot be used to differentiate partial tendon ruptures from focal degenerative lesions.