|
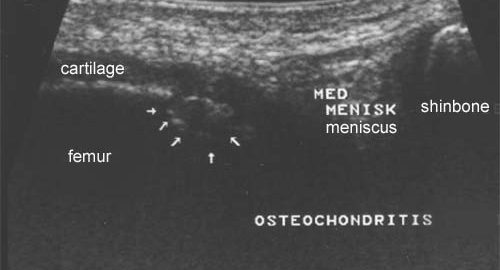
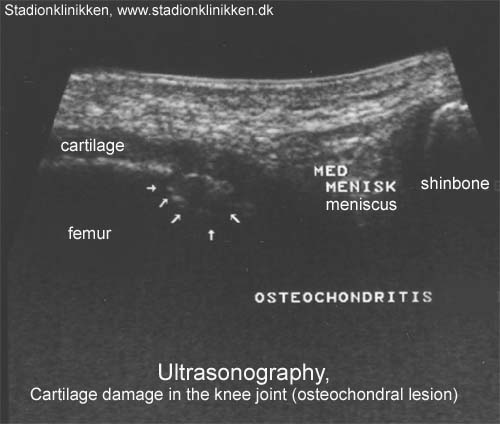
Treatment algorithm for osteochondral injuries of the knee.
Cain EL, Clancy WG. Clin Sports Med 2001 Apr;20(2):321-42
The treatment of osteochondral fractures and OCD lesions in the knee is controversial. Many new procedures and techniques have been developed recently to address osteochondral lesions, indicating that no single procedure is accepted universally. Our treatment algorithm is based on the age of the patient, skeletal maturity, and the presence of adequate subchondral bone attached to the chondral lesion. Most nondisplaced lesions in the patient with open physes will heal with conservative treatment. The onset of skeletal maturity indicates a need for a more aggressive treatment approach. If adequate cortical bone is attached to the fragment, drilling of stable lesions, or drilling with fixation of unstable or loose fragments is appropriate. Autologous bone graft can be necessary to stimulate healing and properly reconstruct the subchondral bony contour. For failed fixation attempts or lesions not amenable to fixation, each treating surgeon must be proficient and comfortable with an articular surface reconstruction technique. The goal for the reconstructive procedure, to produce a smooth gliding articular surface of hyaline or hyaline-like cartilage, is possible using current techniques including mosaicplasty, osteochondral allograft transplantation, and autologous chondrocyte transplantation. Debridement, drilling, microfracture, and abrasion chondroplasty have been shown to result in fibrocartilage with inferior mechanical properties when compared with hyaline cartilage. No long-term studies have been published, however, to confirm the benefits of replacing osteochondral defects with hyaline cartilage rather than fibrocartilage. Although the results of many reconstructive procedures are quite encouraging with early follow up, the ultimate goal is to prevent long-term degenerative arthritis. Only well-designed prospective studies with long-term follow up will determine the adequacy of these procedures in reaching the ultimate goal. This treatment algorithm is based on the senior author’s (WGC) experience with the complex dilemma of osteochondral lesions of the knee.
|