|
Technical pitfalls of collateral ligament surgery. |
Kategoriarkiv: Inner collateral ligament rupture
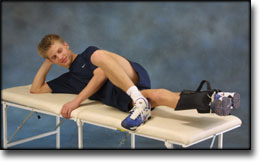
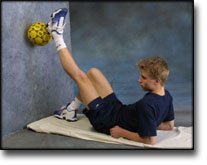
STEP3
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR RUPTURE OF THE INNER COLLATERAL LIGAMENT
(RUPTURA COLLATERALE LIGAMENTUM MEDIALE/TIBIALE)
STEP 3 |
Unlimited: Cycling. Swimming. Running with increasing speed and cautious directional change.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||























| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
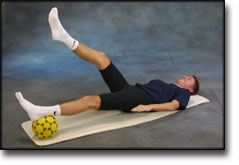
STEP4
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR RUPTURE OF THE INNER COLLATERAL LIGAMENT
(RUPTURA COLLATERALE LIGAMENTUM MEDIALE/TIBIALE)
STEP 4 |
Unlimited: Cycling. Swimming. Running and spurting with sudden directional change and jumping.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||



| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
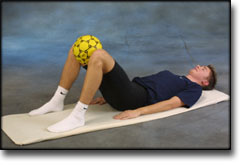
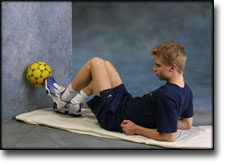
STEP1
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR RUPTURE OF THE INNER COLLATERAL LIGAMENT
(RUPTURA COLLATERALE LIGAMENTUM MEDIALE/TIBIALE)
STEP 1 |
Unlimited: Cycling with raised saddle.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||









| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
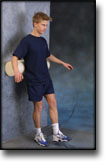
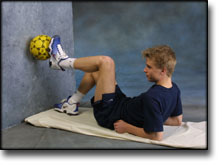
STEP2
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR RUPTURE OF THE INNER COLLATERAL LIGAMENT
(RUPTURA COLLATERALE LIGAMENTUM MEDIALE/TIBIALE)
STEP 2 |
Unlimited: Cycling. Swimming. Light jogging.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||







| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |
treatment-article2
|
Ligament lesions of the knee joint in childhood |
treatment-article1
|
Operative versus non-operative treatment of recent injuries to the ligaments of the knee. A prospective randomized study. |
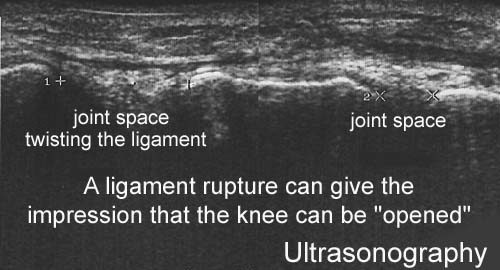
ultrasonic-image

internal side-instability-test
examination-article1
|
Ligament lesions of the knee joint in childhood |