|
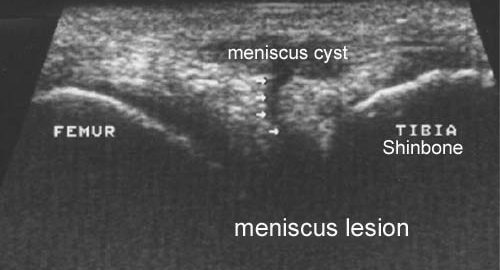
3-dimensional ultrasound in clinical diagnosis of meniscus lesions.
Riedl S, Tauscher A, Kuhner C, Gohring U, Sohn C, Meeder PJ. Ultraschall Med 1998 Feb;19(1):28-33.
AIM.
To compare the significance of the two-dimensional and three-dimensional sonography in the diagnosis of meniscal tears under clinical conditions.
METHODS.
Sixty menisci of knees with clinical symptoms (44 medial and 16 lateral menisci) were examined by an identical transducer in a two- and three-dimensional sonography technique. The findings were compared with the diagnosis made with subsequent arthroscopy.
RESULTS.
In the diagnosis of meniscal lesions the two- and three-dimensional sonography reached a sensitivity of 92% and 100% and a specificity of 83% and 88%, respectively. The positive predictive value of these methods was 58% and 67%. The negative predictive value was 98% and 100%. Because of the good results with the two-dimensional sonography, there were no statistically significant differences between both methods. The three-dimensional sonography, however, proved to be superior, to the two-dimensional sonography in the analysis of subgroups (medial and lateral menisci, menisci with and without clinical symptoms). The negative predictive value of the three-dimensional sonography was 100% for all of these subgroups.
CONCLUSION.
Although this study shows no significant difference in the results of two- and three-dimensional sonography, the analysis of subgroups displays a slightly improved significance for diagnosis of meniscal tears by three-dimensional sonography. The high negative predictive value shows that three-dimensional sonography, performed by an experienced examiner, may be useful to exclude meniscal tears. This result may help focus further cost-intensive or invasive examinations.
|