|
Patellar tendinosis (jumper’s knee): findings at histopathologic examination, US, and MR imaging. Victorian Institute of Sport Tendon Study Group.
Khan KM, Bonar F, Desmond PM, Cook JL, Young DA, Visentini PJ, Fehrmann MW, Kiss ZS, O’Brien PA, Harcourt PR, Dowling RJ, O’Sullivan RM, Crichton KJ, Tress BM, Wark JD. Radiology 1996 Sep;200(3):821-7.
PURPOSE.
To determine the histopathologic findings of patellar tendinosis (“jumper’s knee”) demonstrated with ultrasonography (US) and magnetic resonance (MR) imaging.
MATERIALS AND METHODS.
Twenty-four athletes (28 knees) with jumper’s knee (23 men, one women; mean age, 30.9 years) scheduled to undergo open tenotomy underwent US patellar tendon examination. Seventeen patients (19 knees) also underwent MR imaging. Tissue was obtained for histopathologic examination in all 28 cases. Eleven age-, height-, and weight-matched athletes (22 knees) without previous knee symptoms served as control subjects for the US examination. Control material for histopathologic examination was obtained in 20 cadavers (39 knees). Data were analyzed with standard statistical methods.
RESULTS.
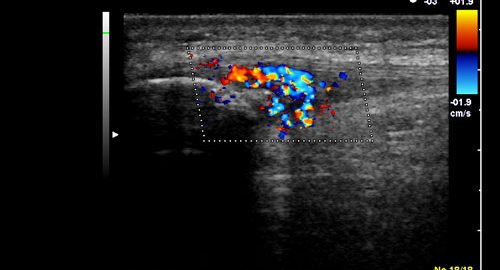
MR imaging and US both revealed an abnormal zone at the proximal patellar tendon attachment. Histopathologic examination revealed mucoid degeneration in all tendons in patients and in 8% (three of 39) of tendons in cadavers (P < .01).
CONCLUSION.
Jumper’s knee is characterized by consistent changes at MR imaging, US, and histopathologic examination and is appropriately described as patellar tendinosis.
|