Training ladder for: IMPINGEMENT SYNDROME IN THE SHOULDER (IMPINGEMENT)
STEP 4
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Bend your injured arm behind your head and using the opposite hand, pull the elbow of the injured arm towards the opposite shoulder so that you feel increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair holding the back of your hands under the lower part of the back. Press your elbows forwards and inwards so that the muscles on the back of the shoulder joint become increasingly stretched. Hold the position for 20 seconds and follow by pressing the elbows backwards so that increased stretching occurs on the front of the shoulder joint. Hold the position for 20 seconds.
(50 min)
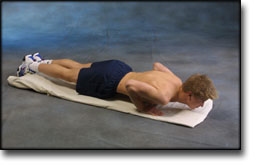
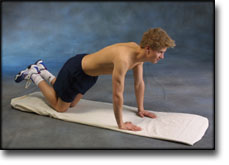
Lie on the floor with instep stretched. Support on your toes and do push-ups without your stomach touching the floor.
Lie on your stomach on a bench or table with the injured arm hanging over the edge. Raise the injured arm stretched horizontally while drawing the shoulder blade in towards your body. A weight or bottle can be held in the hand to increase the load.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand with the good shoulder against a wall. Hold the elastic with the injured arm and move the outstretched arm to the side and away from your body so that the elastic becomes taut.
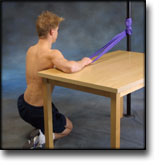
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
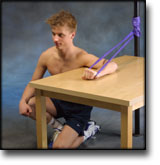
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Stand with the elastic under your foot. Hold the elastic with the injured arm and draw your shoulder upwards. The arm should be kept stretched in against your body the whole time.
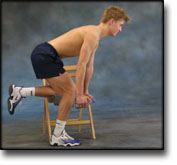
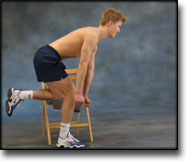
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards holding a weight or a filled bottle. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. Using heavier objects or weights can increase the load.
Stand holding a firm round cushion against the wall with the injured arm. Slowly move the cushion up the wall above 90 degrees.
Stand with your side against a wall holding the elastic with the injured arm. Stretch the elbow with the upper arm at 90 degrees to your body and the hand above shoulder height. Draw the arm downwards and in over your stomach.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: IMPINGEMENT SYNDROME IN THE SHOULDER (IMPINGEMENT)
STEP 3
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair holding the back of your hands under the lower part of the back. Press your elbows forwards and inwards so that the muscles on the back of the shoulder joint become increasingly stretched. Hold the position for 20 seconds and follow by pressing the elbows backwards so that increased stretching occurs on the front of the shoulder joint. Hold the position for 20 seconds.
(50 min)
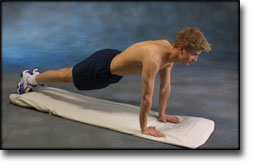
Go down on all fours. Lift your toes from the floor and do push-ups.
Hold an elastic band with the injured arm at a 90-degree angle from the body. Slowly draw the elastic towards yourself so that it tightens.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand with the good shoulder against a wall. Hold the elastic with the injured arm and move the outstretched arm to the side and away from your body so that the elastic becomes taut.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: IMPINGEMENT SYNDROME IN THE SHOULDER (IMPINGEMENT)
STEP 1
The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
Unlimited: Cycling. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair holding the back of your hands under the lower part of the back. Press your elbows forwards and inwards so that the muscles on the back of the shoulder joint become increasingly stretched. Hold the position for 20 seconds and follow by pressing the elbows backwards so that increased stretching occurs on the front of the shoulder joint. Hold the position for 20 seconds.
(50 min)
Support with both hands against a wall. Put your weight on your hands and draw your shoulder blades backwards and forwards.
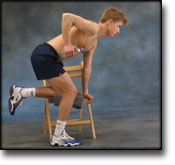
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. You can bend your arm if you have difficulty in locating the shoulder blade muscles.
Stand with your arms outstretched at your sides with the palms of your hands facing forwards. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
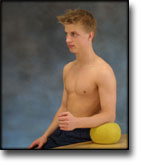
Sit at a table with the injured arm’s elbow on a ball. Press against the ball with a slow movement for 5 seconds. Rest for 5 seconds before repeating.
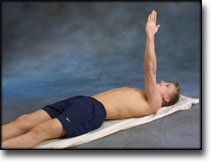
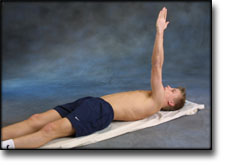
Lie on your back with the injured arm pointing upwards. Stretch the arm further up so that the shoulder blade lifts from the floor, and go down again. The arm must be outstretched the whole time.
Lift both shoulders slowly upwards and down again.
Stand bending forward and supporting a chair back with one hand. Let the other arm hang freely downwards holding a weight. Move the shoulder backwards and forwards and from side to side. It is important that the arm hangs straight down the whole time.
Stand with the injured arm stretched down against your body. First move the arm out from your body 20 degrees and back again, and then out 40 degrees and back again. Finally move the arm out 60 degrees from your body and back again.
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards holding a weight or a filled bottle. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. Using heavier objects or weights can increase the load.
Stand at a table with the injured arm on a ball. Move the ball in all directions while applying slight pressure on the ball.
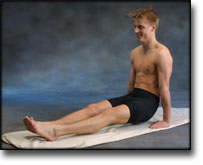
Sit on the floor with outstretched legs. Support with both hands on the floor, and lift yourself by using your arms. Both arms should be stretched.
Hold the elastic with the injured arm with your upper arm alongside your body with the elbow bent. Stretch your arm forwards so that the elastic tightens.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: IMPINGEMENT SYNDROME IN THE SHOULDER (IMPINGEMENT)
STEP 2
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair holding the back of your hands under the lower part of the back. Press your elbows forwards and inwards so that the muscles on the back of the shoulder joint become increasingly stretched. Hold the position for 20 seconds and follow by pressing the elbows backwards so that increased stretching occurs on the front of the shoulder joint. Hold the position for 20 seconds.
(50 min)
Support with both hands against a wall. Move slowly towards the wall and push away again. The exercise is performed like standing push-ups.
Stand with the elastic under your foot. Hold the elastic with the injured arm and draw your shoulder upwards. The arm should be kept stretched in against your body the whole time.
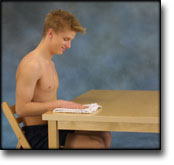
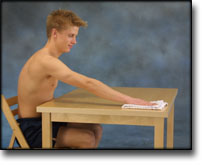
Sit with the injured arm on a table with your hand on a cloth. Polish the tabletop backwards and forwards while applying slight pressure with your arm.
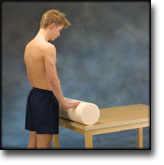
Stand at a table with both hands on a firm round cushion with elbows slightly bent. Apply slight pressure to the cushion and roll the cushion away from yourself so that the upper body bends in over the table. Roll the cushion back again to the starting position.
Stand with the injured arm against a wall with elbow bent. Press the arm against the wall and hold the pressure for 10 seconds. Rest for 10 seconds before repeating. Repeat the exercise 10 times.
Stand and bounce a ball on the floor backwards and forwards from the injured to the good hand.
Hold an elastic band with the injured arm, with the arm by your side and the elbow bent. Slowly draw the elastic towards yourself so that the elastic tightens. The elbow must be bent the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stand with the injured arm stretched down against your body. Move your arm out from your body to maximum 90 degrees.
Lie on your stomach on a bench or table with the injured arm hanging over the edge holding a weight or bottle. Slowly draw the hand up to the shoulder joint.
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
In a cadaver study the success of injections in the subacromial space and acromioclavicular joint was studied. Twenty-four shoulders were dissected after separate dye injection was performed with the patient in the supine position. Subacromial bursa injection was successful in 83% (20 shoulders), but in 15 shoulders other structures were also infiltrated, including seven injections in the rotator cuff. Acromioclavicular joint injection was successful in 67% (16 shoulders), but half involved other structures. The authors believe that misplaced injections may be diagnostically misleading and potentially harmful.
Ultrasonographic diagnosis of the pathology of the rotator cuff and subacromial bursa: criteria.
Fernandes MS, Pinto AC. Acta Med Port 1994 Apr;7(4):211-20.
Shoulder soft tissues echographic evaluation depends on the availability of well established echographic diagnostic criteria, which hasn’t been fully accepted until nowadays, as results in that field have been controversial. The main purpose of the present study has been to determine the echographic criteria of the most frequent shoulder periarticular soft tissue pathology. A prospective study has been carried out, comparing the right to the left shoulder of 37 normals in order to determine the normal characteristics and limits of the selected echographic parameters (echogenicity, echostructure, dimensions in terms of width, rhythm of movement and rotator cuff competence ratio). Afterwards, the relative role of these variables in the identification of three different nosological groups determined through suitable gold standard diagnostic methods (36 suprasinatus tears, 20 supraspinatus tendinitis and 22 subacromial bursitis) has been determined. Lastly, the discriminant power of some echographic parameters association was tested, thus suggesting the echographic criteria to be selected. Results support the following criteria: 1) supraspinatus tears: cuff competence ratio less than 1, the difference value between the affected and the sound tendon thickness less than -1,8 mm associated with asymmetries of one of the remaining parameters (echogenicity, echostructure or rhythm); 2) supraspinatus tendinitis: the difference between the affected and the sound tendon thickness bigger than 1 mm associated with asymmetries of one of the remaining parameters (echogenicity, echostructure or rhythm); cuff competence ratio equal or above 1;3) subacromial bursitis: the difference between the affected and the sound bursa thickness bigger than 1 mm associated with asymmetries of one of the following parametres: echogenicity, echostruture or rhythm.
Internal impingement in the shoulder of the overhand athlete: pathophysiology, diagnosis, and treatment.
Meister K. Am J Orthop 2000 Jun;29(6):433-8.
The etiology of rotator cuff disease is multifactorial in nature. The process by which the articular surface of the rotator cuff can become diseased secondary to direct abutment against the glenoid rim and labrum has been termed internal impingement. Damage to the undersurface of the rotator cuff can occur from contact at the extremes of shoulder motion and can increase secondary to adaptive changes in bone and soft tissue. Diagnosis is achieved in most instances by a thorough physical examination. Adjunctive tests, particularly magnetic resonance imaging, can increase the accuracy of the diagnosis. If this disease is recognized early, nonoperative intervention may be successful. When nonoperative treatment fails, the use of arthroscopy for the treatment of torn rotator cuff and labral tissue and capsular laxity may be indicated to resolve symptoms and restore the premorbid level of function.
Internal impingement was first described by Walch in 1992 and defined as contact between the supraspinatus tendon and posterior-superior glenoid rim with the shoulder in the cocked, throwing position of 90 degrees of abduction and maximum external rotation. The hypothesis of the study was that this contact may be seen in patients who are not throwing athletes nor in those who have instability. One hundred five consecutive patients who underwent shoulder arthroscopy were prospectively studied with preoperative history and physical examination. All patients underwent general anesthesia and arthroscopy with a standard posterior portal. With the patient under arthroscopy the arm was placed in abduction and external rotation until contact was made or until full elevation was reached. Eighty-five percent (N = 90) of the patients made contact between the rotator cuff and glenoid rim at an average of 95 degrees of abduction and 74 degrees of external rotation. No statistically significant relationship was seen (P > .05) between the position of contact at internal impingement and mechanism of injury, throwing versus nonthrowing, instability, rotator cuff tear, preoperative external rotation, or preoperative impingement signs. The intraoperative finding of contact of the rotator cuff to the posterosuperior glenoid with the arm in abduction and external rotation can occur in a wide spectrum of shoulder disease and is not limited to the throwing athlete. Not all patients with increased laxity and instability demonstrate this contact, suggesting that these factors may not be essential for internal impingement.