Training ladder for: LUXATION OF THE JOINT BETWEEN THE SHOULDER BLADE AND THE COLLARBONE (LUXATIO ARTICULI ACROMIOCLAVICULARE)
STEP 4
Unlimited: Cycling. Swimming. Running.
(10 min)
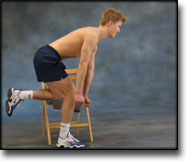
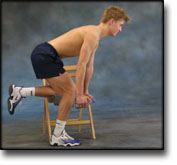
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Bend your injured arm behind your head and using the opposite hand, pull the elbow of the injured arm towards the opposite shoulder so that you feel increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
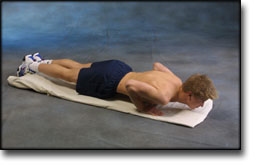
Lie on the floor with instep stretched. Support on your toes and do push-ups without your stomach touching the floor.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Stand with the elastic under your foot. Hold the elastic with the injured arm and draw your shoulder upwards. The arm should be kept stretched in against your body the whole time.
Lie on your stomach on a bench or table with the injured arm hanging over the edge. Raise the injured arm stretched horizontally while drawing the shoulder blade in towards your body. A weight or bottle can be held in the hand to increase the load.
Lie on your stomach on a bench or table with the injured arm hanging over the edge holding a weight or bottle. Slowly draw the hand up to the shoulder joint.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand with the good shoulder against a wall. Hold the elastic with the injured arm and move the outstretched arm to the side and away from your body so that the elastic becomes taut.
Stand with your side against a wall holding the elastic with the injured arm. Stretch the elbow with the upper arm at 90 degrees to your body and the hand above shoulder height. Draw the arm downwards and in over your stomach.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: LUXATION OF THE JOINT BETWEEN THE SHOULDER BLADE AND THE COLLARBONE (LUXATIO ARTICULI ACROMIOCLAVICULARE)
STEP 3
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Bend your injured arm behind your head and using the opposite hand, pull the elbow of the injured arm towards the opposite shoulder so that you feel increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
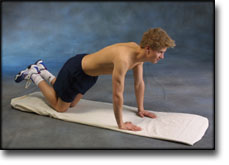
Go down on all fours. Lift your toes from the floor and do push-ups.
Hold an elastic band with the injured arm at a 90-degree angle from the body. Slowly draw the elastic towards yourself so that it tightens.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand with the good shoulder against a wall. Hold the elastic with the injured arm and move the outstretched arm to the side and away from your body so that the elastic becomes taut.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: LUXATION OF THE JOINT BETWEEN THE SHOULDER BLADE AND THE COLLARBONE (LUXATIO ARTICULI ACROMIOCLAVICULARE)
STEP 2
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Bend your injured arm behind your head and using the opposite hand, pull the elbow of the injured arm towards the opposite shoulder so that you feel increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
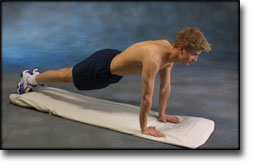
Support with both hands against a wall. Move slowly towards the wall and push away again. The exercise is performed like standing push-ups.
Lift both shoulders slowly upwards and down again.
Hold an elastic band with the injured arm, with the arm by your side and the elbow bent. Slowly draw the elastic towards yourself so that the elastic tightens. The elbow must be bent the whole time.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Hold the elastic with the injured arm with your upper arm alongside your body with the elbow bent. Stretch your arm forwards so that the elastic tightens.
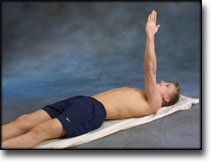
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand and bounce a ball on the floor backwards and forwards from the injured to the good hand.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: LUXATION OF THE JOINT BETWEEN THE SHOULDER BLADE AND THE COLLARBONE (LUXATIO ARTICULI ACROMIOCLAVICULARE)
STEP 1
The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
Unlimited: Cycling. Running.
(10 min)
Sit on a chair with your arms outstretched behind your back with hands together. Lift your arms up and backwards so that the front of the shoulders becomes increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Sit on a chair with one hand on your head and the other holding the chair seat. Slowly draw your head to the side while resisting with the opposite arm so that the muscles on the side of the neck become increasingly stretched. Draw your head in different directions so that all the muscles around the neck are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
(50 min)
Support with both hands against a wall. Put your weight on your hands and draw your shoulder blades backwards and forwards.
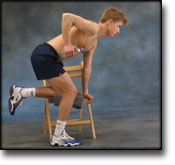
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. You can bend your arm if you have difficulty in locating the shoulder blade muscles.
Stand with your arms outstretched at your sides with the palms of your hands facing forwards. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
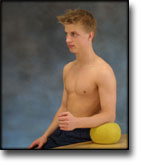
Sit at a table with the injured arm’s elbow on a ball. Press against the ball with a slow movement for 5 seconds. Rest for 5 seconds before repeating.
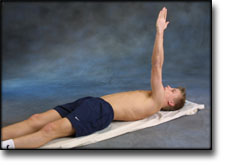
Lie on your back with the injured arm pointing upwards. Stretch the arm further up so that the shoulder blade lifts from the floor, and go down again. The arm must be outstretched the whole time.
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards holding a weight or a filled bottle. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. Using heavier objects or weights can increase the load.
Stand bending forward and supporting a chair back with one hand. Let the other arm hang freely downwards holding a weight. Move the shoulder backwards and forwards and from side to side. It is important that the arm hangs straight down the whole time.
Stand with the injured arm stretched down against your body. First move the arm out from your body 20 degrees and back again, and then out 40 degrees and back again. Finally move the arm out 60 degrees from your body and back again.
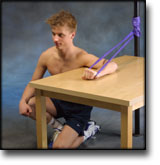
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
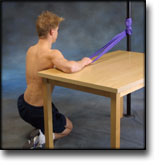
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Surgical treatment of acute, complete acromioclavicular joint dislocation. Indications, technique and results.
Fremerey RW, Lobenhoffer P, Bosch U, Freudenberg E, Tscherne H. Unfallchirurg 1996 May;99(5):341-5.
From June 1983 to May 1990, 51 patients were operated on for acute, complete acromioclavicular dislocation (Tossy III). The operative technique includes suturing of the coracoclavicular and acromioclavicular ligaments and stabilization of the clavicle with resorbable, 10-mm coracoclavicular PDS banding. Six patients received primary resection of the lateral end of the clavicle due to significant injury of the AC joint cartilage. Forty-two patients with an average follow-up of 6.1 years were evaluated clinically using the UCLA and Constant-Murley Score, as well as subjective grading. Additional radiological assessment was performed in 36 cases. Excellent or good clinical results were obtained in 97.6%, with 85.7% being free of pain. All patients with primary resection of the lateral end of the clavicle had no pain. The incidence of postoperative complications was low (one deep wound infection with removal of the PDS band, three secondary dislocations). Post-traumatic arthritis developed in 14.7% of the patients. In those cases of acute grade III AC joint dislocations where operative treatment is indicated, this technique provides excellent results with a low complication rate.
Conservative treatment of acromioclavicular dislocation. Evaluation of functional and radiological results after six years follow-up.
Mulier T, Stuyck J, Fabry G. Acta Orthop Belg 1993;59(3):255-62.
Fifty-eight patients with acute acromioclavicular dislocations of Type III, IV and V (Rockwood classification) were examined to assess the late results of conservative treatment. The average age of the patients was 31 years, and the interval between injury and final review was 6.3 years. Seventy-nine percent of the patients had excellent or good late results. Surprisingly the age and activity level of the patients did not influence our late results, nor did the radiological appearance of acromioclavicular osteoarthritis or periarticular calcification. The radiological appearance of the acromioclavicular joint improved in 41% of patients. In 10 failed cases, excision of the distal end of the clavicle with reconstruction of the coracoclavicular ligament (Weaver and Dunn procedure) resulted in 90% excellent or good results after a 3-year follow-up. A high percentage of excellent results can be expected after this procedure, as long as it is correctly performed.