|
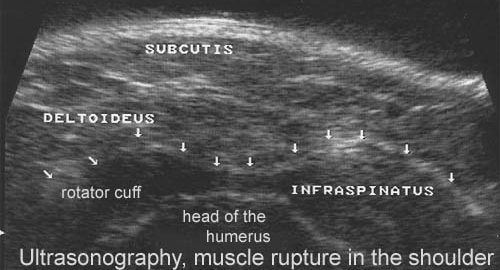
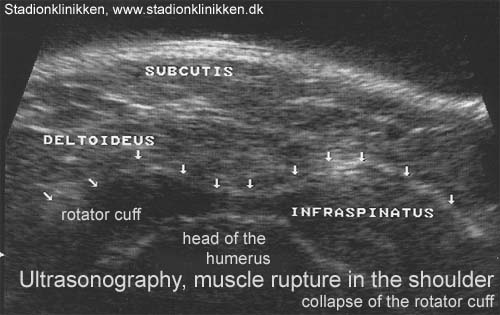
Sonographic signs of complete rotator cuff tears.
Chiou HJ, Hsu CC, Chou YH, Tiu CM, Jim YF, Wu JJ, Chang CY. Chung Hua I Hsueh Tsa Chih (Taipei) 1996 Dec;58(6):428-34.
BACKGROUND.
To evaluate the usefulness of high resolution ultrasound (HRUS) in the examination of complete rotator cuff tear (RCT).
METHODS.
A prospective study of 157 patients with sonographic examination of shoulder was performed. All of them complained of chronic shoulder pain and were referred by clinician for suspicion of RCT. Their age ranged from 30 to 76 years. The ultrasonic scanners we used were Acuson 128 XP 10 with 7MHz linear transducer, or Diasonics VST master series using 10MHz linear transducer. Examination positions included external rotation of shoulder for scanning biceps tendon and subscapularis tendon, and internal rotation for supraspinatus tendon and lateral scan of infraspinatus tendon and teres minor tendon. Sonographic criteria of complete RCT included 1. complete absence of rotator cuff (RC); 2. focal thinning of RC; 3. focal hypoechoic cleft of RC; 4. focal depression of RC; and 5. heterogeneous hypoechoic RC with subdeltoid bursa fluid. Arthrography was performed after sonography examination on the same day.
RESULTS.
Among 49 complete RCTs diagnosed by sonography, 46 were proved to be complete RCT by arthrography; only 3 were false positive. In 108 patients with normal rotator cuff diagnosed by sonography, 104 had compatible results with arthrography; only 4 patients turned out to be complete RCT. The sensitivity, specificity, positive predictive values, negative predictive values and accuracy were 92%, 97.2%, 93.9%, 96.3% and 95.5%, respectively.
CONCLUSIONS.
HRUS can directly demonstrate the morphological changes of RC. It has a high sensitivity and specificity in the diagnosis of complete RCT, and can be used as a firstline screening modality for complete RCT in patients with chronic shoulder pain.
|