TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR MUSCLE RUPTURE IN THE POSTERIOR THIGH (RUPTURA MUSCULI)
STEP 4
The following rehabilitation program will cover the needs for the vast majority of children with muscle rupture in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming. Running and spurting.
(5 min)
Lie on your back. Draw the injured leg up towards your head so that the muscles in the back of the thigh become increasingly stretched. Perform the exercise with outstretched as well as bent knee. Hold the position for 20 seconds and relax for 20 seconds before repeating. The exercise can also be performed standing with the injured leg outstretched on a chair while the upper body is bent slightly forwards.
(40 min)
Sit on a chair with elastic around the ankle, facing the elastic. Lift the leg and slowly bend and stretch the knee.
Stand by a chair with your weight on the healthy leg and a sandbag around the injured leg. Slowly bend and stretch in the injured leg’s knee.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR MUSCLE RUPTURE IN THE POSTERIOR THIGH (RUPTURA MUSCULI)
STEP 3
The following rehabilitation program will cover the needs for the vast majority of children with muscle rupture in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming. Running with increasing speed.
(5 min)
Lie on your back. Draw the injured leg up towards your head so that the muscles in the back of the thigh become increasingly stretched. Perform the exercise with outstretched as well as bent knee. Hold the position for 20 seconds and relax for 20 seconds before repeating. The exercise can also be performed standing with the injured leg outstretched on a chair while the upper body is bent slightly forwards.
(15 min)
Sit on a chair with elastic around the ankle, facing the elastic. Lift the leg and slowly bend and stretch the knee.
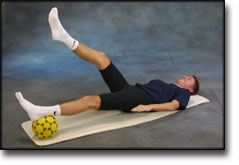
Lie on your back with a ball or firm round cushion under the injured leg. Lift your backside up from the floor and stretch the healthy leg. Hold the position for a few seconds.
Stand by a chair with your weight on the healthy leg and a sandbag around the injured leg. Slowly bend and stretch in the injured leg’s knee.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR MUSCLE RUPTURE IN THE POSTERIOR THIGH (RUPTURA MUSCULI)
STEP 2
The following rehabilitation program will cover the needs for the vast majority of children with muscle rupture in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming. Jogging.
(5 min)
Lie on your back. Draw the injured leg up towards your head so that the muscles in the back of the thigh become increasingly stretched. Perform the exercise with outstretched as well as bent knee. Hold the position for 20 seconds and relax for 20 seconds before repeating. The exercise can also be performed standing with the injured leg outstretched on a chair while the upper body is bent slightly forwards.
(10 min)
Sit on a chair with elastic around the ankle, facing the elastic. Lift the leg and slowly bend and stretch the knee.
Lie on your back with a ball or firm round cushion under both feet. Roll the ball backwards and forwards in a steady pace while lifting your backside.
Stand by a chair with your weight on the healthy leg and a sandbag around the injured leg. Slowly bend and stretch in the injured leg’s knee.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS: FOR MUSCLE RUPTURE IN THE POSTERIOR THIGH (RUPTURA MUSCULI)
STEP 1
The following rehabilitation program will cover the needs for the vast majority of children with muscle rupture in the anterior thigh. Older teenagers involved in sports at a high level can advantageously use the rehabilitation program for adults.
Unlimited: Cycling. Swimming.
(5 min)
Lie on your back. Hold your knee and draw it up against your chest so that the muscles in the back of the thigh become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
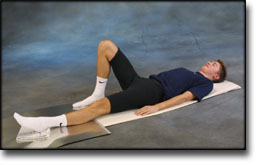
Lie on your back with the heel of the injured leg resting on the bench or a smooth floor. Bend and stretch the injured leg while keeping contact with the surface at all times.
Lie on your stomach on the floor with your arms above your head and with outstretched legs. Lift right arm and left leg together, changing to lift left arm and right leg together.
Lie on your back and bend the injured leg. Lift the healthy leg, and then raise your backside with the weight on the injured leg to be trained. Hold the position a few seconds and lower your backside again. Moving the injured leg further away from the body will increase the load.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
MR imaging in the prognostication of hamstring injury. Work in progress.
Pomeranz SJ, Heidt RS Jr. Radiology 1993 Dec;189(3):897-900.
PURPOSE. To correlate morphologic and magnetic resonance (MR) imaging findings in hamstring injury with short-term prognosis and convalescence interval (CI).
MATERIALS AND METHODS. A retrospective study of 14 professional athletes with hamstring injury was performed. The injuries were categorized according to muscle group involved, percentage of cross-sectional area affected, location, and signal intensity on T1- and T2-weighted spin-echo images.
RESULTS. Longer CIs (> 6 weeks) were seen in injuries with complete transection, greater than 50% cross-sectional muscle involvement, ganglionlike fluid collections (long T1 and T2), hemorrhagelike signal intensity (short T1 and T2), distal myotendinous junction tears, and deep muscular tears. Shorter CIs (< 5 weeks) were seen in superficial muscle injuries and muscle belly injuries that involved small cross-sectional areas of the muscle.
CONCLUSION. Prediction of CI for high-performance athletes with complete hamstring injury may be accomplished with use of MR imaging and poor prognostic factors.