|
||
|
||
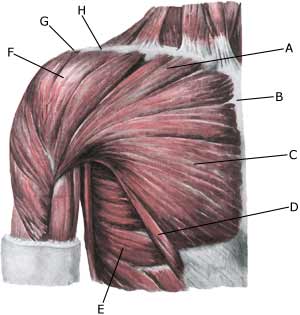
| Cause: When a muscle is subjected to a load beyond the strength of the muscle (fitness training, weight lifting, wrestling), a rupture occurs. The vast majority of ruptures in athletes are total. The rupture is usually located at the anchor on the humerus.
Symptoms: In light cases a local tenderness is felt after the load (“muscle strain”, “imminent pulled muscle”). In severe cases a sudden jolting pain is felt in the muscle (partial “muscle rupture” or “pulled muscle”) and in the worst case a violent snap, rendering the muscle unusable (“total muscle rupture”). In muscle injuries the following three symptoms are characteristic: pain upon pressure, stretching and activation against resistance. In total ruptures a defect can often be seen and felt at the forward fold in the armpit. Acute treatment: Click here. Examination: In light cases with only minimal tenderness and no inconveniences with normal usage of the arm, medical examination is not necessarily required. Though the severity of the tenderness is not always a measure of the severity of the injury. In case of more pronounced tenderness or pain medical examination is required to ensure the diagnosis and treatment. A normal medical examination is usually sufficient in order to make the diagnosis. Pain will be present when pressure is applied to the damaged and deteriorated muscle, when the arm is squeezed to the body against resistance (adduction) and when the muscle is stretched. If there is uncertainty regarding the diagnosis, the medical examination should be supplemented with an ultrasound or MRI scan, which is the most suitable examinations to ensure the diagnosis (article). Treatment: In athletes with total ruptures located at the point of attachment on the humerus, most advise surgery (article). If the rupture is not total or if the rupture is in the muscle belly, relief and careful rehabilitation is recommended. In total ruptures a rehabilitation period stretching over several months must be expected before maximal loading can be resumed. Rehabilitation naturally depends on the degree of rupture and the treatment (conservative / operative). It is advised to avoid fitness training the first couple of months, and hereafter resume it with a very low load so as not to rupture the muscle again. Complications: If progress is not smooth, it should be considered whether the diagnosis is correct or whether complications have arisen. Amongst others the following should be considered:
|