|
||
|
||
 |
||
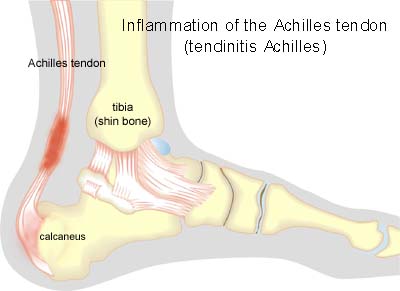
| Cause: Inflammation occurs with continued overload in the form of running and jumping. The risk of over-load injuries of the Achilles tendon increases with age.
Symptoms: Pain when activating the Achilles tendon (running and jumping), when applying pressure and with stretching of the tendon. The tendon often feels thickened. Examination: Medical examination is not necessarily required in slight, early cases where the tenderness is slowly increasing without sudden worsening. In cases when there is a sense of a “crack”, or sudden shooting pains in the Achilles tendon, medical attention should be sought as soon as possible to exclude a (partial) rupture of the Achilles tendon or rupture of the soleus muscle. This situation is best determined by use of ultrasound scanning, as a number of injuries requiring treatment can easily be overlooked during a normal clinical examination. In all cases where satisfactory progress is not in evidence, an ultrasound examination should be performed as early as possible. Ultrasound scanning enables an evaluation of the extent of the change in the tendon; inflammation of the tendon (tendinitis), development of cicatricial tissue (tendinosis), clacification, inflammation of the tissue surrounding the tendon (peritendinitis), inflammation of the bursa (bursitis), as well as (partial) rupture (article) (Ultrasonic image). Treatment: Treatment is primarily comprised of relief from the painful activity (running). If the treatment is commenced early, the injury can in some cases heal within a few weeks. If the pain has been experienced for several months, and if ultrasound scanning has revealed thickening of, and changes in the tendon, a rehabilitation period of several months must be anticipated. Relief and cautious stretching will be sufficient to calm the symptoms in the majority of young athletes. In more severe, lengthy or repeated cases in teenagers, emphasis is put on fitness training where the tendon is activated simultaneously with stretching (eccentric training) (article). It is naturally crucial that footwear is in good condition (good running shoes with shock absorbing heel and close fitting heel cap). Pressure on the Achilles tendon can be relieved by using shoes with an elevated heel, whilst a heel cushion in the shoe is of less significance since the heightening achieved by this method is greatly limited. If experiencing tenderness in the Achilles tendon during the rehabilitation period, treatment with ice for a period of at least 20 minutes is recommended. Bandage: Taping to relieve problems with the Achilles tendon is of questionable significance, but can be attempted as the tape will not invoke further injury if applied in the correct manner (tape-description). Complications: If there is not a steady improvement in the condition an ultrasound scan should be performed to exclude:
|