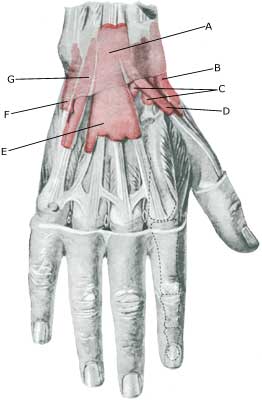
INFLAMMATION OF THE TENDON SHEATH ON THE OUTER WRIST
|
||
|
||
| Cause: Inflammation of the tendon sheath (tenosynovitis) occurs as a result of mechanical irritation of the tendon sheath due to repeated uniform movements of the tendon, causing the tendon to become inflamed and swell (article).
Symptoms: Slowly commencing pain along the wrist on the side of the thumb. The area can occasionally feel swollen, and crackling sensation felt upon movement of the thumb. The pain deteriorates when twisting a rag, and when the thumb is moved away from the index finger against resistance. Acute treatment: Click here. Examination: Slight cases do not necessarily require medical examination. The doctor should be consulted if there is lack of progress despite relief. The diagnosis is usually made from a normal medical examination, however, in the event of doubt in connection with the diagnosis an ultrasound scan can be performed which will easily and quickly detect the inflammation (Ultrasonic image) (article). Treatment: The treatment primarily involves relief, stretching and strength training of the muscles around the wrist. It is imperative for the treatment that the triggering load factor is reduced (article). In cases with a lack of progress following relief, a medical treatment can be considered in the form of rheumatic medicine (NSAID) or the injection of corticosteroid in the tendon sheath. Since the effect and the risk is dependant on the injection being performed correctly, the injection can advantageously be executed under ultrasound guidance. Surgery is rarely indicated. Bandage: It will often relieve the injury if a wrist splint is used. Complications: If there is a lack of progress it should be considered if the diagnosis is correct or whether complications have arisen: |