|
||
|
||
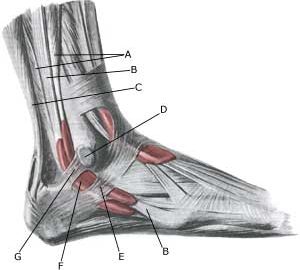
| Cause: Discomfort can be produced if a rupture of the connective tissue (retinaculum musculorum peroneorum superius & inferius) behind the outer ankle knuckle (malleolus lateralis) occurs. A rupture of the connective tissue (retinaculum) is relatively often combined with outer ligament injuries in the ankle joint.
Symptoms: Pain at the outer ankle knuckle (malleolus lateralis), where certain movements of the ankle joint can give rise to a painful sense of “slipping”. Acute treatment: Click here. Examination: When the painful movement of the ankle joint is performed, normal examination can detect the tendon slip over the outer ankle knuckle. A normal medical examination is usually sufficient in order Treatment: Treatment is primarily concentrated on providing rest from the painful activities (running). If steady progress from rest and rehabilitation is not achieved, and ultrasound scanning reveals inflammation of the tendon sheath, the treatment can be supplemented by medicinal treatment in the form of rheumatic medicine (NSAID) Alternatively, draining and evaluating fluid can be performed, and injection of corticosteroid into the tendon sheath. Injection into the tendon sheath is best performed if ultrasound guided. Surgical intervention can be attempted in certain cases, if resting, rehabilitation and medicinal treatment do not provide the desired result (article). Complications: If there is not a steady improvement in the condition consideration must be given as to whether the diagnosis is correct, or if complications have arisen:
Possibly supplement with further examinations (x-ray, ultrasound scanning). |
