|
||
|
||
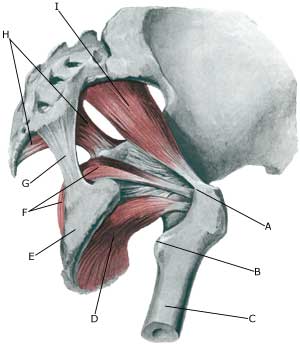
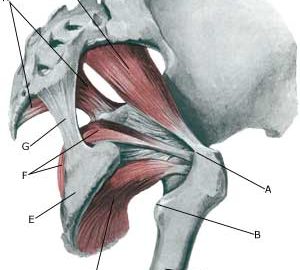
| Cause: If the muscle is over-loaded, it will become taut and tender. In some cases, the muscle can become so taut that it jams against the ischias nerve (nervus ischiadicus).
Symptoms: Pain deep in the buttock, with periodic radiation into the leg. Examination: The diagnosis will be rendered probable under clinical examinations by demonstrating tenderness by applying pressure on the muscle deep within the buttock, as well as provoking pain by stretching and activating the muscle. There is no suitable method to provide a pictorial image of the muscle (MR scanning can be attempted in the event of suspicions of nerve impingement) (article). Treatment: The treatment usually comprises stretching and subsequent strength training of the muscles surrounding the lower back and buttocks. It is only in very rare cases involving nerve impingement that surgery is indicated. Uncomfortable pain can be treated medicinally in the form of paracetamol, or possibly rheumatic medicine (NSAID) . If this treatment does not provide the desired relief, ultrasound guided injection of corticosteroid in the most tender part of the muscle can be attempted (article 1), (article 2). Special: Shock absorbing shoes or inner inlays will reduce the risk of various forms of muscle infiltrations. In the event of unsatisfactory progress, or relapse after successful rehabilitation, consideration must be given to performing an analysis of the patient’s running style to establish whether a correction of the running style should be recommended. Complications: If progress is not smooth, the correctness of the diagnosis should be considered or whether complications have arisen. The following should be considered in particular:
|