OBJECTIVE: This investigation evaluated a novel form of tissue perfusion measurement, laser Doppler imaging (LDI), in a case of lateral epicondylitis to establish if it might have applications in assessing soft tissue lesions. LDI was used in conjunction with ultrasonography to provide information about tissue oedema as well as the power Doppler signal as an alternative method of assessing blood flow. METHODS: A laser Doppler imager with a near-infrared (NIR) laser source was used to improve tissue penetration and yield measurements of perfusion (flux) from structures under the skin. Skin temperature over the lateral epicondylar region was also measured. Ultrasonography was used in both grey-scale and power Doppler modes. LDI, temperature measurements and ultrasonographic data were obtained before treatment and serially after local injection of methylprednisolone. RESULTS: Before treatment there was increased perfusion and skin temperature and the presence of a power Doppler sign associated with the right lateral epicondyle as well as oedema at the extensor origin. None of these was present at the asymptomatic contralateral epicondylar region. Twenty-four hours after methylprednisolone administration, both perfusion and skin temperature had increased, and they declined over the subsequent 48 h. Although skin temperature had declined to normal (referenced to the contralateral epicondyle) by the third day after injection, it took until the eleventh day after injection for perfusion to normalize. CONCLUSIONS: LDI using an NIR laser source appears to be an effective non-invasive method for the examination of inflammatory responses in soft tissue, with greater sensitivity than thermally based methods. In addition, LDI was found to correlate with power Doppler ultrasonography.
We describe two cases of bursitis at the insertion of the biceps tendon. They presented as swellings in the cubital fossa with symptoms of median nerve irritation. The aetiology was probably mechanical trauma; both patients were cured by operation.
Supracondylar Fractures of the Humerus in Children.
Otsuka NY, Kasser JR. J Am Acad Orthop Surg 1997 Jan;5(1):19-26.
The treatment of type II and type III supracondylar fractures of the humerus in children with closed reduction and percutaneous pinning has dramatically lowered the rate of complications from this injury. The incidence rates of malunion (cubitus varus) and compartment syndrome have both decreased. Nerve injury accompanying this type of fracture (prevalence, 5% to 19%) is usually a neurapraxia, which should be managed conservatively. Vascular insufficiency at presentation (prevalence, 5% to 17%) should be managed initially by rapid closed reduction and pinning without arteriography. Persistent vascular insufficiency necessitates exploration and vascular reconstruction.
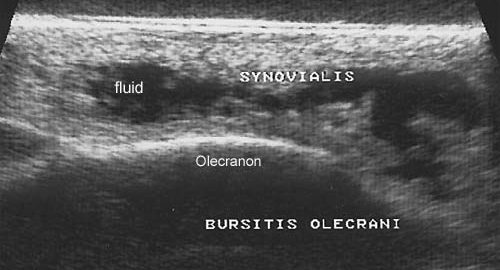
Septic and non-septic olecranon bursitis in the accident and emergency department–an approach to management.
Stell IM. J Accid Emerg Med 1996 Sep;13(5):351-3.
Olecranon bursitis is relatively common. One third of episodes are septic. Most of the remainder are non-septic, with occasional rheumatological causes. Trauma can cause both septic and non-septic olecranon bursitis. Clinical features are helpful in separating septic from non-septic olecranon bursitis, but there may be local erythema in both. Aspiration should be carried out in all cases, and if the presence of infection is still in doubt, microscopy, Gram staining, and culture of the aspirate will resolve the issue. Septic olecranon bursitis should be treated by aspiration, which may need to be repeated, and a long course of antibiotics. Some cases will need admission, and a few will need surgical treatment. Non-septic olecranon bursitis can be managed with aspiration alone. Non-steroidal anti-inflammatory drugs probably hasten symptomatic improvement. Intrabursal corticosteroids produce a rapid resolution but concern remains over their long term local effects. Recovery from septic olecranon bursitis can take months.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 4
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Cycling. Running. Swimming.
(10 min)
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
Stand and bounce a ball on the floor backwards and forwards from the injured to the good hand.
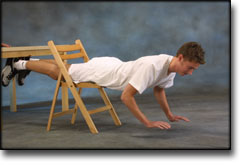
Lie on your stomach across a chair with both feet supported under a tabletop. Lift both hands from the floor and hold the position for 2 seconds. Support with your hands for 2 seconds and repeat the exercise 10 times in quick succession.
Support with both hands against a wall. Move slowly towards the wall and push away again. The exercise is performed like standing push-ups.
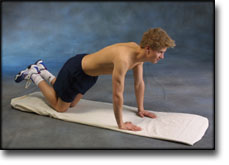
Go down on all fours. Lift your toes from the floor and do push-ups.
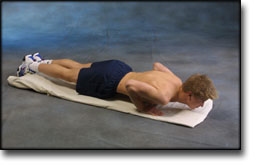
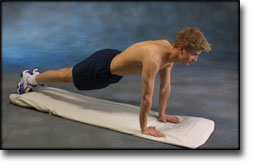
Lie on the floor with instep stretched. Support on your toes and do push-ups without your stomach touching the floor.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 3
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Cycling. Running. Swimming.
(10 min)
Rotate the forearm so that the palm faces alternately up and down.
Bend and stretch the arm to the extreme position. Cautiously apply pressure in the extreme position to achieve maximum mobility.
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
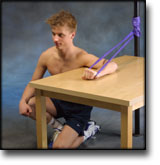
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
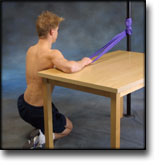
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 2
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Running. Cycling.
(20 min – Primarily to achieve full mobility)
Rotate the forearm so that the palm faces alternately up and down.
Bend and stretch the arm to the extreme position. Cautiously apply pressure in the extreme position to achieve maximum mobility.
(40 min)
Stand holding a firm round cushion against the wall with the injured arm. Slowly move the cushion up the wall above 90 degrees.
Lie on your stomach across a table or chair and support with both arms on the floor. Raise one arm from the floor and hold the position for approx. 10 seconds. Change arm.
Lie on your back with support at the elbow. Slowly bend and stretch the elbow while holding a weight.
Lie on your stomach on a bench or table with the injured arm hanging over the edge holding a weight or bottle. Slowly draw the hand up to the shoulder joint.
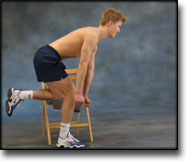
Stand slightly bent over a chair, with your weight on the good arm and the injured arm hanging loosely downwards. Lift your arm/shoulder upwards by using the shoulder blade’s muscles. You can bend your arm if you have difficulty in locating the shoulder blade muscles.
Sit at a table holding a hammer in the injured hand, with the arm resting on the table and the hand over the edge. Slowly rotate the lower arm from side to side.
Using an elastic band around the back of the injured hand, move the wrist upwards while keeping the elastic taut.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: TRAINING LADDER FOR TRAINING LADDER FOR DISCLOCATION OF THE ELBOW (LUXATIO ARTICULI CUBITI)
STEP 1
This rehabilitation program should only be considered in connection with an uncomplicated dislocation of the elbow, that has not required surgery. The rehabilitation to be followed must be agreed with your doctor if complications have arisen in the form of, for example, bone fracture, vascular damage or nerve damage.
Unlimited: Running.
(20 min – Primarily to achieve full mobility)
Rotate the forearm so that the palm faces alternately up and down.
Bend and stretch the arm to the extreme position. Cautiously apply pressure in the extreme position to achieve maximum mobility.
(40 min)
Squeeze a soft ball.
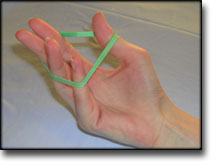
Put an elastic band around your fingers. Spread your fingers so that the elastic is stretched.
Stand at a table with the injured arm on a ball. Move the ball in all directions while applying slight pressure on the ball.
Let the injured hand hang over the edge of a table with the palm facing downwards. Move the hand slowly up and down while holding a weight. Support the injured arm with the good arm.
Sit at a table with the injured hand on a ball and roll slowly from side to side.
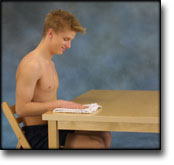
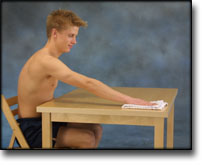
Sit with the injured arm on a table with your hand on a cloth. Polish the tabletop backwards and forwards while applying slight pressure with your arm.
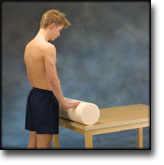
Stand at a table with both hands on a firm round cushion with elbows slightly bent. Apply slight pressure to the cushion and roll the cushion away from yourself so that the upper body bends in over the table. Roll the cushion back again to the starting position.
Sit at a table with the injured arm’s elbow on a ball. Press against the ball with a slow movement for 5 seconds. Rest for 5 seconds before repeating.
Sit at a table with the injured hand on a ball and roll slowly backwards and forwards.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.