Training ladder for: RUPTURE OF MUSCLE ON THE FRONT OF THE UPPER ARM (RUPTURA MUSCULI BICEPS BRACHII)
STEP 4
Unlimited: Cycling. Swimming. Running.
(10 min)
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
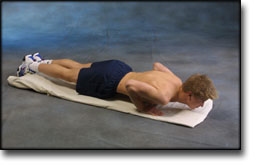
Lie on the floor with instep stretched. Support on your toes and do push-ups without your stomach touching the floor.
Lie on your stomach on a bench or table with the injured arm hanging over the edge holding a weight or bottle. Slowly draw the hand up to the shoulder joint.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand with the good shoulder against a wall. Hold the elastic with the injured arm and move the outstretched arm to the side and away from your body so that the elastic becomes taut.
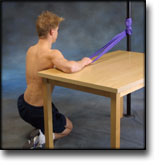
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand with your side against a wall holding the elastic with the injured arm. Stretch the elbow with the upper arm at 90 degrees to your body and the hand above shoulder height. Draw the arm downwards and in over your stomach.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: RUPTURE OF MUSCLE ON THE FRONT OF THE UPPER ARM (RUPTURA MUSCULI BICEPS BRACHII)
STEP 3
Unlimited: Cycling. Swimming. Running.
(10 min)
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
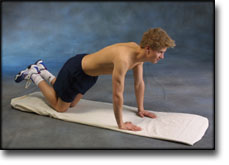
Go down on all fours. Lift your toes from the floor and do push-ups.
Hold an elastic band with the injured arm at a 90-degree angle from the body. Slowly draw the elastic towards yourself so that it tightens.
Put the elastic under your foot, and with the injured arm draw the other end upwards by bending your arm.
Hold the elastic with the injured arm with elbow bent and your hand at shoulder level. Stretch your arm forwards so that the elastic is tightened.
Stand with your side against a wall. Hold the elastic with the injured arm with elbow bent, upper arm 90 degrees away from your body and your hand at shoulder height. The palm of your hand should face the floor. Drawn your arm downwards and in front of your stomach.
Stand with the elastic under your foot. Hold the elastic with the injured arm and drawn the arm slowly back and upwards so that the elastic is taut.
Stand with the good shoulder against a wall. Hold the elastic with the injured arm and move the outstretched arm to the side and away from your body so that the elastic becomes taut.
Kneel facing the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the palm facing the wall and move your elbow up and down.
Kneel facing away from the wall with the injured arm on a table. The tabletop must be at shoulder height. Hold the elastic with the back of your hand facing the wall and move your elbow up and down.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: RUPTURE OF MUSCLE ON THE FRONT OF THE UPPER ARM (RUPTURA MUSCULI BICEPS BRACHII)
STEP 2
Unlimited: Cycling. Running.
(10 min)
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
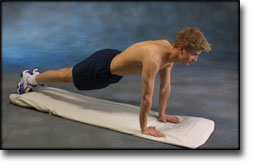
Support with both hands against a wall. Move slowly towards the wall and push away again. The exercise is performed like standing push-ups.
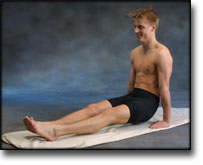
Sit on the floor with outstretched legs. Support with both hands on the floor, and lift yourself by using your arms. Both arms should be stretched.
Hold an elastic band with the injured arm, with the arm by your side and the elbow bent. Slowly draw the elastic towards yourself so that the elastic tightens. The elbow must be bent the whole time.
Hold an elastic band in the good arm. Take hold of the other end of the elastic with the injured arm and draw the injured arm downwards.
Hold the elastic with the injured arm with your upper arm alongside your body with the elbow bent. Stretch your arm forwards so that the elastic tightens.
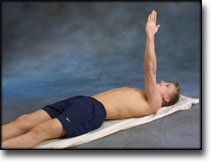
Lie on your back with the injured arm raised upwards. Hold the elastic between your hands with the good arm against your chest. Stretch the injured arm further upwards so that the shoulder blade lifts from the floor.
Stand with the elastic under your foot. Hold the elastic with the injured arm and draw your shoulder upwards. The arm should be kept stretched in against your body the whole time.
Stand and bounce a ball on the floor backwards and forwards from the injured to the good hand.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm outwards so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stand holding the elastic with the upper arm against your body and elbow bent at 90 degrees. Twist your lower arm in over your stomach so that the elastic is taut and draw your arm slowly back again. The elbow must be held against your body the whole time.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Training ladder for: RUPTURE OF MUSCLE ON THE FRONT OF THE UPPER ARM (RUPTURA MUSCULI BICEPS BRACHII)
STEP 1
The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
Unlimited: Cycling. Running.
(10 min)
Stand in a doorframe. Press your arms against the frame so that the front of your shoulders become increasingly stretched. Move your arms up and down the doorframe so that different parts of your muscles are stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with your hands together behind your back. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
Stand with the injured arm in front of your body. With the opposite hand, press the elbow of the injured arm towards the opposite shoulder, so that the upper part of the arm and the outer shoulder experiences increased stretching. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(50 min)
Support with both hands against a wall. Put your weight on your hands and draw your shoulder blades backwards and forwards.
Stand with your arms outstretched at your sides with the palms of your hands facing forwards. Draw your shoulder blades together (imagine trying to hold a pencil between your shoulder blades). Hold the position for 10 seconds and rest for 10 seconds before repeating.
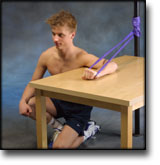
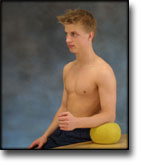
Sit at a table with the injured arm’s elbow on a ball. Press against the ball with a slow movement for 5 seconds. Rest for 5 seconds before repeating.
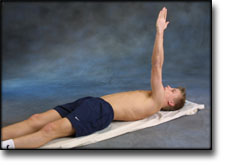
Lie on your back with the injured arm pointing upwards. Stretch the arm further up so that the shoulder blade lifts from the floor, and go down again. The arm must be outstretched the whole time.
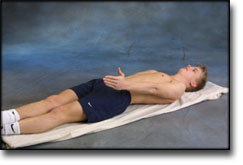
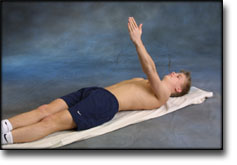
Lie on your back with the injured arm by your side. Move the arm up and over your head before slowly retuning the arm again. The arm must be outstretched the whole time.
Lift both shoulders slowly upwards and down again.
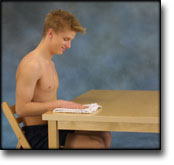
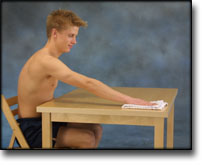
Sit with the injured arm on a table with your hand on a cloth. Polish the tabletop backwards and forwards while applying slight pressure with your arm.
Stand with the injured arm stretched down against your body. Move your arm out from your body to maximum 90 degrees.
Stand with the injured arm against a wall with elbow bent. Press the arm against the wall and hold the pressure for 10 seconds. Rest for 10 seconds before repeating. Repeat the exercise 10 times.
Stand at a table with the injured arm on a ball. Move the ball in all directions while applying slight pressure on the ball.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Biceps tendon: diagnosis, therapy and results after proximal and distal rupture.
Klonz A, Reilmann H. Orthopade 2000 Mar;29(3):209-15.
Ruptures of the long head of the M. biceps humeri are commonly caused by degenerative changes within the tendon. They are associated with pathologies of the subacromial space. The loss of power regarding elbow flexion and supination amounts to 8 to 21% after conservative treatment. Refixation offers a small but evident improvement of flexion and supination power. Especially endurance is improved. The number of cases with remaining light or marked weakness is reduced by more than 50%. Deformity by the slipped muscle can be corrected effectively. Function of the glenohumeral joint can only be improved if associated subacromial problems are identified and treated simultaneously. As complications are uncommon surgery should be recommended to young and active patients and should at least be offered to less active patients. Ruptures of the distal tendon are less common. Thirteen patients were re-examined after operative repair for distal biceps tendon avulsion and 277 reported cases were reviewed. After conservatie management (n = 20) the power of flexion will remain reduced by 30%-40%, that of supination by more than 50%. The loss of flexion power, as well as the deformity can be diminished by attachment of the distal biceps to the brachialis muscle (n = 22). The anatomic re-insertion (n = 248) additionally reduces the loss of supination power to 0%-25%, but bears a higher risk of complications. Using the ‘double-incision technique’ (n = 105 of 248) does not decrease the risk of naval lesions but increases the incidence of radioulnar synostosis. The use of suture anchors provides a nice way of fixation of the tendon but does not facilitate the approach to the tuberosity. The distal biceps tendon rupture should be treated operatively. The adequate method of repair is to be determined individually.
Management of acute and chronic biceps tendon rupture.
Aldridge JW, Bruno RJ, Strauch RJ, Rosenwasser MP. Hand Clin 2000 Aug;16(3):497-503.
In conclusion, the authors believe that younger high-demand patients should be offered the option of surgical repair; can be performed through the preferred single anterior incision with two suture anchors. Chronic tears, even with retraction, may be successfully reconstructed using a free tendon graft, often the flexor carpi radialis. Complications, including radial nerve palsy and proximal radioulnar synostosis, can be avoided with the single-incision technique. Older, low-demand patients can be rehabilitated and have excellent function without acute repair. Partial tendon injuries, for the most part, may be treated with rest and rehabilitation and explored only for chronic, unremitting pain. The authors believe that the single anterior approach should be used over the previously popularized two-incision technique.
Durr HR, Stabler A, Pfahler M, Matzko M, Refior HJ. Clin Orthop 2000 May;(374):195-200.
Partial rupture of the distal biceps tendon is a relatively rare event, and various degrees of partial tendon tears have been reported. In the current study four patients with partial atraumatic distal biceps tendon tears (mean age, 59 years; range, 40-82 years) are reported. In all four patients, a common clinical pattern emerged. Pain at the insertion of the distal biceps tendon in the radius unrelated to any traumatic event was the main symptom. In all patients the diagnosis was based on magnetic resonance imaging or computed tomography imaging. In three of four patients the partial rupture of the tendon caused a significant bursalike lesion. The typical appearance was a partially ruptured biceps tendon, with contrast enhancement signaling the degree of degeneration, tenosynovitis, and soft tissue swelling extending along the tendon semicircular to the proximal radius. In three patients, conservative treatment was successful. Only one patient needed surgery, with reinsertion of the tendon resulting in total functional recovery.
PURPOSE. To review the authors’ experience with magnetic resonance (MR) imaging of patients with suspected injury of the distal biceps tendon.
MATERIALS AND METHODS. Twenty-one patients with clinically suspected injury of the distal biceps tendon were evaluated with MR imaging. Surgical correlation was performed in 15 patients, and long-term clinical follow-up was performed in the remaining six cases.
RESULTS. Twelve complete biceps tears, four partial tears, one brachialis rupture, and one ganglion were identified. Axial MR images were more valuable than sagittal images in accurately grading distal biceps tendon injury preoperatively. There was 100% agreement between MR imaging and surgical findings. MR imaging findings led to changes in clinical treatment plans in eight patients (38%).
CONCLUSION. MR imaging is useful in the evaluation of patients with suspected distal biceps tendon injury. In particular, axial MR images of the distal biceps insertion are important for accurate grading of the injury.