TRAINING LADDER FOR CHILDREN: INFLAMMATION OF THE GROWTH ZONE IN THE ELBOW (LITTLE LEAGUE ELBOW)
STEP 4
The treatment primarily comprises relief. This “treatment” is quite sufficient on most children, and the sports activity can be cautiously resumed when the pain has diminished. The period of relief is usually quite short if the relief treatment is started soon after the onset of the symptoms. The following training program can be used by larger children and teenagers.
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit at a table with the injured arm hanging over the edge with the palm facing downwards. Use the other arm to apply pressure on the back of the injured hand so that the injured lower arm becomes increasingly stretched on the upper side. Repeat the exercise where the injured hand is alternately pressed from side to side. The injured arm should finally be turned over and the exercise repeated by pressing the underside of the hand so that the injured lower arm becomes increasingly stretched on the under side. The stretching positions should be held for 20 seconds followed by 20 seconds of rest before repeating.
Sit on a table holding your arms in to your body. Turn your hands so that the fingers face backwards and thumbs to the side. Your arms should be outstretched. Slowly lean your upper body backwards so that your forearms become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(20 min)
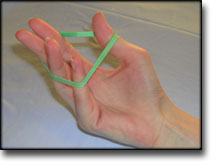
Using an elastic band around the back of the injured hand, move the wrist upwards while keeping the elastic taut.
Sit at a table with the side of the injured hand resting on the table edge. Place the elastic around the thumb, draw it downwards over the back of the hand and hold with the good hand. Slowly rotate the lower arm from side to side to stretch the elastic.
Let the injured hand hang over the edge of a table with the palm facing downwards. Move the hand slowly up and down while holding a weight. Support the injured arm with the good arm.
Lie on your back with support at the elbow. Slowly bend and stretch the elbow while holding a weight.
Squeeze a soft ball.
Put an elastic band around your fingers. Spread your fingers so that the elastic is stretched.
Let the injured hand hang over the edge of a table with the back of the hand facing downwards. Holding a weight, slowly move your hand up and down while supporting the arm with the good hand.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN: INFLAMMATION OF THE GROWTH ZONE IN THE ELBOW (LITTLE LEAGUE ELBOW)
STEP 3
The treatment primarily comprises relief. This “treatment” is quite sufficient on most children, and the sports activity can be cautiously resumed when the pain has diminished. The period of relief is usually quite short if the relief treatment is started soon after the onset of the symptoms. The following training program can be used by larger children and teenagers.
Unlimited: Cycling. Swimming. Running.
(10 min)
Sit at a table with the injured arm hanging over the edge with the palm facing downwards. Use the other arm to apply pressure on the back of the injured hand so that the injured lower arm becomes increasingly stretched on the upper side. Repeat the exercise where the injured hand is alternately pressed from side to side. The injured arm should finally be turned over and the exercise repeated by pressing the underside of the hand so that the injured lower arm becomes increasingly stretched on the under side. The stretching positions should be held for 20 seconds followed by 20 seconds of rest before repeating.
Sit on a table holding your arms in to your body. Turn your hands so that the fingers face backwards and thumbs to the side. Your arms should be outstretched. Slowly lean your upper body backwards so that your forearms become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Using an elastic band around the back of the injured hand, move the wrist upwards while keeping the elastic taut.
Sit at a table with the side of the injured hand resting on the table edge. Place the elastic around the thumb, draw it downwards over the back of the hand and hold with the good hand. Slowly rotate the lower arm from side to side to stretch the elastic.
Let the injured hand hang over the edge of a table with the palm facing downwards. Move the hand slowly up and down while holding a weight. Support the injured arm with the good arm.
Lie on your back with support at the elbow. Slowly bend and stretch the elbow while holding a weight.
Squeeze a soft ball.
Put an elastic band around your fingers. Spread your fingers so that the elastic is stretched.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN: INFLAMMATION OF THE GROWTH ZONE IN THE ELBOW (LITTLE LEAGUE ELBOW)
STEP 2
The treatment primarily comprises relief. This “treatment” is quite sufficient on most children, and the sports activity can be cautiously resumed when the pain has diminished. The period of relief is usually quite short if the relief treatment is started soon after the onset of the symptoms. The following training program can be used by larger children and teenagers.
Unlimited: Cycling. Running.
(10 min)
Sit at a table with the injured arm hanging over the edge with the palm facing downwards. Use the other arm to apply pressure on the back of the injured hand so that the injured lower arm becomes increasingly stretched on the upper side. Repeat the exercise where the injured hand is alternately pressed from side to side. The injured arm should finally be turned over and the exercise repeated by pressing the underside of the hand so that the injured lower arm becomes increasingly stretched on the under side. The stretching positions should be held for 20 seconds followed by 20 seconds of rest before repeating.
Sit on a table holding your arms in to your body. Turn your hands so that the fingers face backwards and thumbs to the side. Your arms should be outstretched. Slowly lean your upper body backwards so that your forearms become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Sit at a table with the injured hand over the edge and the palm facing upwards. Use the good hand to place slight pressure on the injured hand and hold the position for 10 seconds. Rest for 10 seconds before repeating.
Squeeze a soft ball.
Put an elastic band around your fingers. Spread your fingers so that the elastic is stretched.
Curl a tea towel with outstretched arms.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
TRAINING LADDER FOR CHILDREN: INFLAMMATION OF THE GROWTH ZONE IN THE ELBOW (LITTLE LEAGUE ELBOW)
STEP 1
The treatment primarily comprises relief. This “treatment” is quite sufficient on most children, and the sports activity can be cautiously resumed when the pain has diminished. The period of relief is usually quite short if the relief treatment is started soon after the onset of the symptoms. The following training program can be used by larger children and teenagers.
Unlimited: Cycling. Running.
(10 min)
Sit at a table with the injured arm hanging over the edge with the palm facing downwards. Use the other arm to apply pressure on the back of the injured hand so that the injured lower arm becomes increasingly stretched on the upper side. Repeat the exercise where the injured hand is alternately pressed from side to side. The injured arm should finally be turned over and the exercise repeated by pressing the underside of the hand so that the injured lower arm becomes increasingly stretched on the under side. The stretching positions should be held for 20 seconds followed by 20 seconds of rest before repeating.
Sit on a table holding your arms in to your body. Turn your hands so that the fingers face backwards and thumbs to the side. Your arms should be outstretched. Slowly lean your upper body backwards so that your forearms become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Sit at a table with the injured hand over the edge with the palm facing upwards. Bend and stretch the wrist.
Sit at a table with the injured hand over the edge with the palm facing downwards. Bend and stretch the wrist.
Sit at a table with the injured hand over the edge and the palm facing upwards. Use the good hand to place slight pressure on the injured hand and hold the position for 10 seconds. Rest for 10 seconds before repeating.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Local corticosteroid injection in sport: review of literature and guidelines for treatment.
Fredberg U. Scand J Med Sci Sports 1997 Jun;7(3):131-9.
The risks and benefits of local injection therapy of overuse sports injuries with corticosteroids are reviewed here. Injection of corticosteroid inside the tendon has a deleterious effect on the tendon tissue and should be unanimously condemned. No reliable proof exists of the deleterious effects of peritendinous injections. Too many conclusions in the literature are based on poor scientific evidence and it is just the reiteration of a dogma if all steroid injections are abandoned. The corticosteroids represent an adjuvant treatment in the overall management of sports injuries: basic treatment is ‘active’ rest and graduated rehabilitation within the limits of pain. With proper indications there are only few and trivial complications that may occur with corticosteroid injections. Guidelines for proper local injection therapy with corticosteroids are given. (Se hele artiklen)
The elbow is one of the most common sites of overuse injuries in adolescent baseball players. The term “little league elbow” has been used to describe a number of entities. This article reports three cases of painful persistence of the olecranon epiphyseal plate in adolescent pitchers. Symptoms associated with this entity may improve with rest and avoidance of the aggravating activity. However, if symptoms persist and the contralateral growth plate has closed, internal fixation may be necessary and is effective in relieving the symptoms.
A case of an acute traction apophysitis, “little league elbow”, in an adolescent badminton player is presented. After a period of intense badminton activity, the patient developed typical signs of inflammation related to his elbow. X-ray showed soft tissue calcifications and ultrasound showed intra-articular swelling and a possible apophysitis related to the elbow. After a period of immobilization followed by low activity he could return to normal sports activity.
Gugenheim JJ Jr, Stanley RF, Woods GW, Tullos HS. Am J Sports Med 1976 Sep-Oct;4(5):189-200
1. In a study of 595 Little League pitchers, approximately 17% had a history of elbow symptoms: only 1% had elbow symptoms which had ever excluded them from pitching. There was no correlation between the presence of symptoms and years of pitching experience. 2. Some limitation of active extension of the elbow was seen in 12% of the pitchers; however, there was no correlation between elbow flexion contractures and years of pitching experience, symptoms, or roentgenographic pathology. No normal child had an elbow flexion contracture greater than 15 degrees. 3. A slight valgus carrying angle is considered a normal anatomic variant in the dominant arm. There was no correlation between valgus carrying angle and years of pitching experience or symptoms or roentgenographic pathology. 4. No roentgenographic evidence of avascular necrosis of the capitellum, radial head, or both was seen in this population. 5. Roentgenographic findings such as bony hypertrophy, enlargement of the medial epicondyle, and secondary ossification centers are normal anatomic variants not related to symptoms. Undisplaced stress fractures of the medial epicondyle respond well to conservative treatment, with no functional residual.
Loomer RL. Can J Appl Sport Sci 1982 Sep;7(3):164-6
Throwing and racquet sports produce large stresses at the elbow joint consisting of tension on the medial or ulnar side, and compression on the lateral or radial side. Medial tension can lead to tears of the common flexor origin or medial collateral ligament, ulnar nerve subluxation, or pronator teres syndrome. Bony lesions include fragmentation and partial avulsion of the medial humeral epicondyle (little league elbow) or even complete avulsion of the epicondyle. The possible sequelae of excessive lateral compression include osteochondritis dissecans of the capitellum, osteochondral fractures of the capitellum and radius, and loose bodies. Early and accurate diagnosis is essential to initiate proper treatment.