Unlimited: Cycling. Swimming. Running with directional change.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Stand on the leg to be trained. Take-off and land on the same leg.
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
Stand on the injured leg with your upper body bent forwards at 90 degrees. Lift the good leg in a straight line behind you. When you feel comfortable with the exercise, it can be made more difficult by closing your eyes.
(40 min)
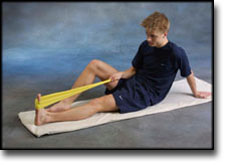
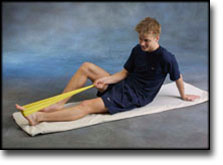
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Up and down from the stool with load. Tie elastic around the hip and go up on the stool in a slow movement. The elastic should be fastened to the wall.
Go up and down from the stool. Go up with alternating right and left legs.
Stand on the healthy leg with elastic fixed around the hip. The elastic should be fixed to the wall or a wall bar. Take-off on the healthy leg and land on the leg to be trained and keep your balance. Remember that the elastic should be positioned so that it gives resistance at the moment of take-off. Change legs.
Stand with both legs on the stool with elastic around the hip. Take-off and land with feet together.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Stand on the leg to be trained. Take-off and land on the same leg.
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
Stand on the injured leg with your upper body bent forwards at 90 degrees. Lift the good leg in a straight line behind you. When you feel comfortable with the exercise, it can be made more difficult by closing your eyes.
(40 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Up and down from the stool with load. Tie elastic around the hip and go up on the stool in a slow movement. The elastic should be fastened to the wall.
Go up and down from the stool. Go up with alternating right and left legs.
Stand on the healthy leg with elastic fixed around the hip. The elastic should be fixed to the wall or a wall bar. Take-off on the healthy leg and land on the leg to be trained and keep your balance. Remember that the elastic should be positioned so that it gives resistance at the moment of take-off. Change legs.
Stand with both legs on the stool with elastic around the hip. Take-off and land with feet together.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
Unlimited: Cycling. Swimming. Light running straight ahead (without directional change) on a smooth surface.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Stand on one leg. Play the ball up against the wall.
Stand on one leg on the floor or a mattress. Look straight ahead and keep the knee slightly bent.
Seesaw. Balance on two legs, possibly using a hand as support against the wall, balancing subsequently on one leg without support. Look straight ahead and keep knees bent.
(40 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Sit on the floor. Tip the foot from side to side with elastic on the inner side of the foot, without moving the knee.
Stand behind a chair. Rise slowly up on tiptoe and go down again.
Up and down from the stool with load. Tie elastic around the hip and go up on the stool in a slow movement. The elastic should be fastened to the wall.
Go up and down from the stool. Go up with alternating right and left legs.
Stand with both legs on the stool with elastic around the hip. Take-off and land with feet together.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
The indications of time after stretching, coordination training and strength training show the division of time for the respective type of training when training for a period of one hour. The time indications are therefore not a definition of the daily training needs, as the daily training is determined on an individual basis.
Unlimited: Cycling. Swimming. Running in deep water.
(10 min)
Stand with the injured leg stretched backwards with the toes facing front. Slowly bend the knee so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand with the injured leg outstretched with the ankle joint bent up against the wall. Press your abdomen against the wall so that the calf muscles become increasingly stretched. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support on the wall with the hand on the same side. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the big toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn slightly outwards so that increased stretching is experienced on the inside of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
Stand on the good leg while gaining support from the wall with the opposite hand. Bend the knee of the injured leg and draw the heel towards the buttocks. Take hold of the little toe side of the foot and draw slowly upwards so that the ankle joint is stretched to the maximum and drawn over the good leg so that increased stretching is experienced on the outer side of the shin bone. Hold the position for 20 seconds and relax for 20 seconds before repeating.
(10 min)
Stand on one leg on the floor or a mattress. Look straight ahead and keep the knee slightly bent.
(40 min)
Sit on the floor. Tip the foot up and down with elastic under the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot up and down with elastic on top of the forefoot so that the elastic becomes taut.
Sit on the floor. Tip the foot from side to side with elastic on the outer side of the foot, without moving the knee.
Stand on a soft surface. Rise slowly up on tiptoe and go down again.
Go up and down from the stool. Go up with alternating right and left legs.
Sit with a ball under the foot. Roll the ball backwards and forwards and from side to side.
Stand on both legs. Tip the toes on the leg to be trained upwards and down again, whilst having the heel firmly on the floor during the exercise.
Sit on a chair. Keep the heel firmly on the ground and tip the toes up.
Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated. The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements.
The neurophysiological and clinical outcomes of surgical decompression of 22 cases of tarsal tunnel syndrome are analysed. Recent work by Pfeiffer & Cracchiolo has suggested a successful outcome in only 44% of cases. We have reviewed the outcome of surgery both clinically and with the use of nerve conduction studies. Pre- and post-operative motor conduction delays in the plantar nerves are compared with clinical results found both in the clinic and later by a postal questionnaire. Despite careful clinical and neurophysiological assessment prior to a full surgical release, only 42% of patients had a satisfactory outcome. A larger reduction in plantar nerve conduction delay post-operatively corresponded well to an improvement in symptoms. However, we were unable to predict which cases would respond to decompression using clinical or electrophysiological methods. We question the use of nerve conduction studies in the diagnosis of tarsal tunnel syndrome, and also the role of surgery in the management of this condition.
The dorsiflexion-eversion test for diagnosis of tarsal tunnel syndrome
Kinoshita M, Okuda R, Morikawa J, Jotoku T, Abe M. J Bone Joint Surg Am 2001 Dec;83-A(12):1835-9
BACKGROUND: The clinical diagnosis of tarsal tunnel syndrome lacks objectivity and consistency. We have devised a new diagnostic physical examination test in which the tibial nerve is compressed as it runs beneath the flexor retinaculum behind the medial malleolus. In this test, the ankle is passively maximally everted and dorsiflexed while all of the metatarsophalangeal joints are maximally dorsiflexed and held in this position for five to ten seconds. METHODS: We performed this test on fifty normal volunteers (100 feet) and on thirty-seven patients (forty-four feet) treated operatively for tarsal tunnel syndrome between 1987 and 1997. We performed the maneuver both preoperatively and postoperatively and recorded any consequent changes in the signs and symptoms; during the operation we observed the altered anatomical relationships in the tarsal tunnel that were produced by the maneuver. The average duration of follow-up was three years and eleven months. RESULTS: Before the operation, the signs and symptoms of tarsal tunnel syndrome were intensified or induced by the maneuver in fifteen of the twenty feet of the patients who reported numbness, in fifteen of the seventeen feet of those who reported pain alone, and in six of the seven feet of those who had combined numbness and pain. Local tenderness was intensified in forty-two of forty-three feet, and it was induced in one foot in which it had been previously absent. A Tinel sign became more pronounced in forty-one feet, and the sign was induced in three feet in which it had been absent previously. During the operation, the tibial nerve was stretched and compressed beneath the laciniate ligament when the ankle was dorsiflexed, the heel was everted, and the toes were dorsiflexed. Preoperative signs and symptoms disappeared on an average of 2.9 months after the operation, and they could not be induced by repeating the test except in three patients, all of whom had tarsal tunnel syndrome subsequent to a fracture of the calcaneus. In the normal volunteers, no symptoms or signs could be induced by the test. CONCLUSION: This new physical examination test is effective in facilitating the diagnosis of tarsal tunnel syndrome.
Tarsal tunnel syndrome: ultrasonographic and MRI features.
Machiels F, Shahabpour M, De Maeseneer M, Schmedding E, Wylock P, Osteaux M. JBR-BTR 1999 Apr;82(2):49-50.
Tarsal tunnel syndrome is a well-known but rare entrapment neuropathy involving the posterior tibial nerve in the tarsal tunnel, a fibro-osseous channel extending from the medial aspect of the ankle to the midfoot. Posttraumatic fibrosis, ganglion cyst, tenosynovitis, tumor of the nerves or other structures, dilated or tortuous veins can cause significant nerve compression in this anatomic region. Herein, we present the typical ultrasonographic and magnetic resonance features of this disorder in patient with a ganglion cyst.