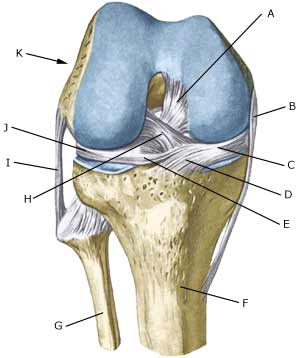
RUPTURE OF THE ANTERIOR CRUCIATE LIGAMENT
|
||
|
||
| Cause: Rupture of the anterior cruciate ligament usually occurs during running with fast changes of direction or as the result of a fall while skiing. Most injuries occur without contact with an opponent.
Symptoms: Usually a snap can be heard or felt and continued sports activity must be aborted. The knee swells within the first few hours, after which the knee can not bend completely. You can subsequently often sense that the leg gives way (knee failure). Acute treatment: Click here. Examination: If a partial or complete rupture of the cruciate ligament is suspected, you should seek medical attention (casualty ward) immediately, to obtain a diagnosis. The doctor can perform various tests on the knee (front drawer looseness, Lachmann, Pivot shift) to examine the stability of the knee. It should be noted that the looseness in the knee can often only be demonstrated after two weeks. The fluid in the knee can be drained. Blood in the knee provides a very strong suspicion of a rupture of the anterior cruciate ligament. The bleeding that occurs after a rupture of the anterior cruciate ligament can usually be seen in an ultrasound scan (Ultrasonic image) (article) or MR-scan. Arthroscopy (a telescopic examination of the knee) is the best suited examination if there is any doubt in the diagnosis. Treatment: Young athletes or others with physically demanding work will usually be advised surgery with the insertion of a new cruciate ligament (article). An intensive rehabilitation period of at least six months is to be expected. It is important that the knee is stretched completely at least twice a day. The surgeon should be consulted if problems occur with stretching the knee completely. Bandage: Hinge bandages (Don-Joy) can be utilised the first few weeks. Tape treatment of cruciate ligament ruptures in the knee has no sure effect. Complications: In case of lack of progress you should consider various complications to the surgery:
In cases where the knee cap tendon is used as a new cruciate ligament an inflammation, is often seen where the knee cap tendon has been removed. With prolonged discomfort which does not diminish following relief, medical treatment in form of rheumatic medicine (NSAID) or injection of corticosteroid along the inflamed part of the knee cap tendon can be attempted (article). Special: Since there is a risk that the injury can cause permanent disability, the injury should be reported to your insurance company. |