IMPINGEMENT SYNDROME IN THE SHOULDER
|
||
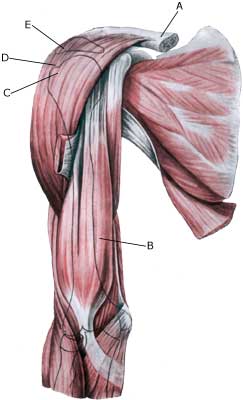
| Cause: There are two main causes for impingement: One external and one internal. The external impingement is usually caused by repeated loads with the arm above the head (tennis, swimming) and causes an inflammation in the upper shoulder blade muscle (M supraspinatus) and the above-lying bursa (bursae subacromialis), which swells and may become squeezed between the head of the humerus (caput humeri) and the upper bone projection of the shoulder blade (acromion), when the arm is raised above the head (see inflammation of the bursa). The internal impingement is caused by the supraspinatus muscle tendon scraping against the edge of the shoulder’s meniscus (posterior-superior edge of the labrum glenoidale) when throwing (90 degrees abduction and maximal extension and outwards rotation), causing damage to both the muscle tendon and the meniscus (article). Symptoms: Slowly insetting local tenderness after the load, externally and to the front of the shoulder. Sometimes radiating down the upper arm. Pain deteriorates when external pressure is applied to the supraspinatus muscle, on the front of the shoulder and when the muscle is brought into contact with the meniscus in the shoulder (throwing exercises) or when the arm is brought approx. 80-120 degrees away from the body (abduction). Acute treatment: Click here. Examination: If no progress is made with relief and discontinuance of the pain inducing activity, a medical examination should be carried out to ensure that the diagnosis is correct and to commence the correct treatment. It is important to make the diagnosis as fast as possible, since the injury may otherwise slowly deteriorated (article). Ordinary medical examination is usually sufficient to make the diagnosis (internal impingement-test: Chicken-wing test), but if there is uncertainty concerning the diagnosis, it should be supplemented with an ultrasound scan, which is the most suitable examination for shoulder injuries (article). Though it is not rare for the diagnosis only being made after a arthroscopic examination is carried out (telescopic examination of the shoulder joint). Treatment: The treatment primarily involves relief from the pain inducing activity, stretching and rehabilitation of the muscles around the shoulder, Impingement syndrome in athletes. In case of lack of progress a medical treatment can be considered, rheumatic medicine (NSAID) or injection of corticosteroid (usually in the subacromiale bursa and possibly in the shoulder joint itself as well (internal impingement with signs of synovitis)). Since the injection of corticosteroid is part of a long-term rehabilitation of a long-term injury, it is often necessary for the rehabilitation period to stretch over several weeks to months in order to reduce the risk of recurrences. Ultrasound guided injections offer the optimal effect with a minimum of risk, (article). In case of lack of progress in the rehabilitation and medical treatment, an operative treatment can be attempted. Complications: If progress is not smooth, it should be considered whether the diagnosis is correct or whether complications have arisen. Amongst others the following should be considered:
|