|
||
|
||
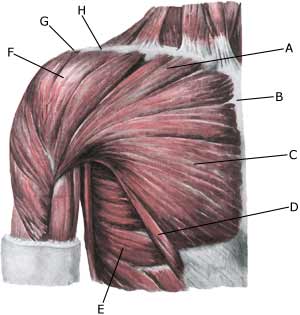
| Cause: When a muscle is subjected to a load beyond the strength of the muscle (butterfly swimming, weight training, weight lifting) a rupture occurs. Most ruptures in athletes are partial ruptures. The rupture can be located both in the front and the back as well as at the attachment to the upper arm (humerus).
Symptoms: In light cases a localised tenderness can be felt following the load (“muscle strain”, “imminent pulled muscle”). In more severe cases sudden shooting pains in the muscle can be felt (“partial muscle rupture”) and in the worst cases a sudden snap is felt, rendering the muscle unusable (“total muscle rupture”) this is very rare, and is almost only seen in conjunction with other damage in the shoulder. With muscle injuries the following three symptoms are characteristic: pain upon pressure, stretching and activating against resistance. Acute treatment: Click here. Examination: Light cases with only minimal tenderness and no discomfort when using the arm do not necessarily require medical examination. The extent of the tenderness is, however, not always a mark of the degree of the injury. In case of more pronounced tenderness medical examination is advised with the aim of securing a correct diagnosis and treatment. Pain will be present when pressure is applied to the damaged muscle, which will be aggravated when the muscle is activated against resistance and when the muscle is stretched. Ultrasound is well suited to ensure the diagnosis. Treatment: The treatment primarily involves relief, discontinuance of the injury inducing activity, stretching and increasing fitness training. Complications: If satisfactory progress is not made, a physician should be consulted to ensure that the diagnosis is correct and that no complications have arisen. Amongst others the following should be considered:
|