|
Sonography of the injured ulnar collateral ligament of the thumb. |
Kategoriarkiv: Arm
Examination
|
The skier’s thumb. |
STEP4
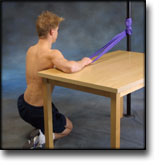
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR DISCLOCATION OF THE ELBOW
(LUXATIO ARTICULI CUBITI)
STEP 4 |
|
||||||||||||||||||||||||||||||||||||



















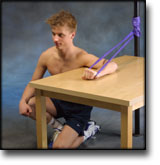
STEP3
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR DISCLOCATION OF THE ELBOW
(LUXATIO ARTICULI CUBITI)
STEP 3 |
|
||||||||||||||||||||||||||||||||||||||||||||||||







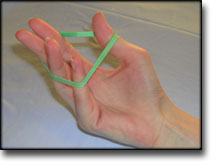
STEP2
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR DISCLOCATION OF THE ELBOW
(LUXATIO ARTICULI CUBITI)
STEP 2 |
|
|||||||||||||||||||||||||||||||||||||||











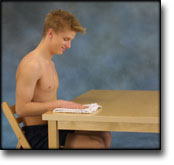
STEP1
TRAINING LADDER FOR CHILDREN AND ADOLESCENTS:
FOR DISCLOCATION OF THE ELBOW
(LUXATIO ARTICULI CUBITI)
STEP 1 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||









Complications
|
Acute elbow dislocation: evaluation and management. |
treatment-article2
|
Return to Australian rules football after acute elbow dislocation: |
treatment-article1
|
Indications for operation in elbow dislocation. |
STEP4
TRAINING LADDER FOR CHILDREN:
INFLAMMATION OF THE GROWTH ZONE
IN THE ELBOW
(LITTLE LEAGUE ELBOW)
STEP 4 |
| The treatment primarily comprises relief. This “treatment” is quite sufficient on most children, and the sports activity can be cautiously resumed when the pain has diminished. The period of relief is usually quite short if the relief treatment is started soon after the onset of the symptoms. The following training program can be used by larger children and teenagers. |
Unlimited: Cycling. Swimming. Running.
|
||||||||||||||||||||||||||||||||||||||||||||









| Stretching is carried out in the following way: stretch the muscle group for 3-5 seconds. Relax for 3-5 seconds. The muscle group should subsequently be stretched for 20 seconds. The muscle is allowed to be tender, but must not hurt. Relax for 20 seconds, after which the procedure can be repeated.
The time consumed for stretching, coordination and strength training can be altered depending on the training opportunities available and individual requirements. |