|
||
|
||
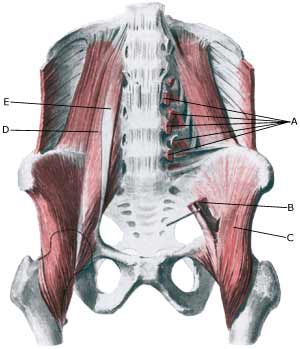
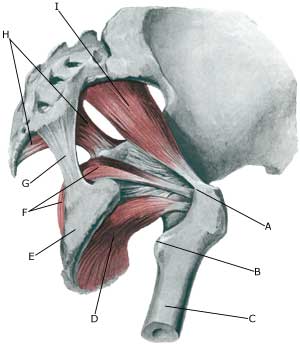
| Cause: In case of repeated loads the muscle tendon can become inflamed, swell and with some movements slip over the one of the bone projections at the pelvis or the hip joint. When the tendon slips over the bone projection, the uncomfortable symptoms are produced. There are three known causes of snapping hips: outer snapping hip (tractus iliotibialis), inner snapping hip (iliopsoas tendon) and joint conditioned (intraarticular) causes (article). The treatment is dependant on the cause.
Symptoms: With certain movements in the hip joint the deep hip flexor (M iliopsoas) can be made to slip over one of the bone projections on the pelvis or the hip joint, whereby a slipping sensation, often accompanied by discomfort, is felt and often heard. Acute treatment: Click here. Examination: In light cases with only minimal tenderness medical examination is not necessarily required. In case of more pronounced pain or lack of progress a medical examination should be carried out to ensure the diagnosis. A normal medical examination is usually sufficient in order to make the diagnosis, however, if there is any doubt concerning the diagnosis a dynamic ultrasound scan can be performed, where the tendon can be seen slipping as this triggers the symptoms (article 1) (article 2), (article 3). Treatment: The treatment primarily comprises relief. If progress is not smooth the treatment can be supplemented with rheumatic medicine (NSAID) or the injection of corticosteroid, which should be done with ultrasound guidance to ensure the optimal effect and minimal risk. Only in very rare cases is surgical treatment necessary. Complications: If progress is not smooth it should be considered whether the diagnosis is correct or if complications have arisen. In particular the following should be considered:
|